Chris Barkley1, Kenneth Bhauti2, Charmaine Natasha Nyakonda3, Devyn E.Z. Lee3, Andrew Dallos3, Katherine G. Merrill4
1 Grassroot Soccer, Inc.
2 Independent Researcher
3 Grassroot Soccer, Inc., Research and Development
4 University of Illinois Chicago, Center for Dissemination and Implementation Science
Citation:
Barkley, C., Bhauti, K., Nyakonda, C.N., Lee, D.E.Z., Dallos, A., & Merrill, K.G. (2026). Grassroot Soccer’s Adolescent Mental Health Programming at Scale: Insights from Routine Monitoring Data across Three African Countries. Journal of Sport for Development. Retrieved from https://jsfd.org/
ABSTRACT
Routine monitoring data are an underused but important source of insight into large-scale, real-world program implementation. Three years into implementing its mental health programme called MindSKILLZ, Grassroot Soccer, an adolescent health organization, initiated a multi-country analysis of its routine monitoring data to: 1) examine MindSKILLZ effects overall, by mental health construct, country, delivery method, and participant characteristics; and 2) gather feedback from experts and youth on the MindSKILLZ pre-post questionnaire to improve its design. Pre-post questionnaire data from 2,286 participants in Kenya, Zambia, and Zimbabwe were analyzed. Results demonstrate statistically significant improvements across countries. Program participants showed substantial gains in stigma reduction (+44.8%), help-seeking (+43.6%), and mental health knowledge (+34.2%). Clinically meaningful improvements in mental well-being were observed in Zimbabwe (+16 points), alongside positive change in Zambia (+6 points). Feedback from experts and youth highlighted challenges with the pre-post questionnaire (e.g., youth comprehension), prompting pre-post tool revisions. Findings demonstrate the value of routine monitoring data for identifying trends in program outcomes and guiding ongoing program improvement. Research studies are needed to establish causal impacts of programming.
INTRODUCTION
In low- and middle-income countries (LMIC), particularly in sub-Saharan Africa (SSA), adolescents experience a disproportionately high burden of mental health difficulties compared to their peers in other regions (Hart & Norris, 2024). A recent systematic review of 37 studies from 16 sub-Saharan African countries (2008–2020) found that adolescents (10–19 years) experience mental health conditions at higher rates than global and other LMIC averages, with 1 in 7 facing significant psychological challenges and 1 in 10 meeting criteria for a psychiatric diagnosis (Jörns-Presentati et al., 2021). Epidemiologic models estimate that the relative disability burden from mental health conditions in SSA will increase by 130% by 2045 (Meffert et al., 2021). Adolescence and young adulthood are particularly critical life stages for mental health, with estimates that 35% of mental health disorders onset by the age of 14 and 75% before the age of 25 years (Kessler et al., 2005; Solmi et al., 2022; Uhlhaas et al., 2023). Without prevention, early detection, and treatment during adolescence, mental health conditions accrue additional comorbidity once they persist into adulthood (Fusar-Poli, 2019).
Universally delivering mental health promotion programs early and through lay providers is one promising strategy for addressing adolescent and youth mental health needs (Chibanda et al., 2011; Sensoy Bahar et al., 2023; Yatham et al., 2018). Early access to youth-friendly, contextually relevant mental health programs is essential to reducing the long-term psychological, social, and economic challenges of mental illness (McGorry & Mei, 2023). There is encouraging evidence that adolescent mental health promotion can improve mental health outcomes (Mabrouk et al., 2022; Skeen et al., 2019). A 2019 global review of 158 studies of universally delivered adolescent mental health interventions found statistically significant positive effects on multiple mental health outcomes, such as reduced depressive symptoms and improved well-being (Skeen et al., 2019). Moreover, a 2022 scoping review of mental health interventions for adolescents in SSA also found positive significant impacts in 55 out of 62 studies that examined intervention effectiveness (Mabrouk et al., 2022).
In addition to the benefits of universally delivered mental health promotion programs, the growing field of sport for development (SFD) offers a promising avenue for strengthening the mental health outcomes of adolescents. SFD programs, which use sport as a means of promoting positive outcomes (Schulenkorf et al., 2016), have shown positive effects on a range of health outcomes in SSA (Hansell et al., 2021). Interventions promoting physical activity can support mental wellbeing through such mechanisms as improved physical self-perceptions and enhanced self-esteem (Lubans et al., 2016). However, evidence for the effects of SFD programs on mental health outcomes has been positive in some cases (Latimer et al., 2025) and negative in others (Richards et al., 2014). SFD programs may negatively affect mental health through pressure and competitive stress and unhealthy coaching practices (Coalter, 2013; Eather et al., 2023), or “negative socialization that constrict a person’s identities, relationships, and experiences” (Coakley, 2011, p. 3). Furthermore, we know little about universally delivered SFD programs addressing adolescent mental health at scale across diverse SSA contexts. Much available evidence on mental health promotion programming, broadly, continues to come from high-income countries (HICs), often based on small-scale interventions tested under controlled research conditions (Skeen et al., 2019; Yatham et al., 2018).
In this context, this paper presents an analysis of Grassroot Soccer’s mental health programming delivered to 2,286 adolescents from Kenya, Zambia, and Zimbabwe. Grassroot Soccer (GRS) is an adolescent health organization that uses a positive youth development approach, play-based education, and near-peer mentors to improve health and promote well-being. Since its founding in 2002, GRS has reached over 25 million young people with its evidence-based SKILLZ programs and has demonstrated program effects through numerous studies on such topics as HIV prevention, gender-based violence, substance use, and mental health (Barkley et al., 2025; Clark et al., 2006; Kaufman et al., 2012; Lee et al., 2025; Merrill et al., 2018; Rotheram-Borus et al., 2016). In 2022, GRS designed a mental health strategy, which included plans to develop a mental health promotion program, called MindSKILLZ (Lee et al., 2025).
Three years into the delivery of MindSKILLZ across three countries, GRS conducted a thorough analysis of its routine monitoring data. Routine monitoring data offer an underutilized but valuable means of understanding program implementation at scale in real-world settings (Berkel et al., 2019; UNDP Evaluation Office, 2002). Analysis of routine monitoring data can facilitate cross-contextual learning about how programming works and shed light on potential program effects on desired outcomes. It provides an opportunity to identify patterns across participants’ characteristics (e.g., age, gender) and context-specific variations (e.g., country) such that program teams can make data-informed decisions about ongoing delivery. Routine monitoring can further involve relevant parties to improve routine monitoring tools, for instance, by clarifying which outcomes are useful (Centre for Effective Services, 2022).
This analysis focused on three countries where MindSKILLZ was delivered between January 1, 2022 and December 31, 2024: Kenya, Zambia, and Zimbabwe. GRS runs its programs directly in Zambia through its affiliate-program model and supports partner organizations with running its programs in Kenya and Zimbabwe. Adolescents in these countries face large unmet mental health needs (Das-Munshi et al., 2016; Doyle et al., 2023; Longwe et al., 2025). To generate actionable insights on the MindSKILLZ program’s performance to inform future program design and implementation, a multi-country analysis of GRS’s routine MindSKILLZ monitoring data was conducted with two aims:
- Examine effects of the mental health program overall, by mental health construct, country, delivery method, and participant characteristics;
- Gather feedback from experts and youth on the MindSKILLZ pre-post questionnaire to improve its design.
MindSKILLZ Program Overview
MindSKILLZ is Grassroot Soccer’s SFD mental health promotion program for adolescents ages 10–19. The program is grounded in Bandura’s Social Learning Theory (Bandura, 1977), which proposes that individuals acquire new behaviors by observing others, not only through direct experience. People are more likely to model behaviors demonstrated by individuals they perceive as similar to themselves. Guided by this principle, GRS recruits trained near-peer mentors they call “Coaches” from the same communities as participants. Through comprehensive training, these Coaches learn social and emotional skills, and model positive, health-promoting behaviors that influence the attitudes and behaviors of participants (Bandura, 1986).
MindSKILLZ is delivered to groups of 20-30 adolescents, typically facilitated by pairs of Coaches using a semi-structured Coach’s Guide. Sessions use play-based learning and group discussions to increase mental health awareness, reduce stigma, strengthen coping skills, and promote help-seeking behaviours. The program was developed through a review of global best practices in adolescent mental health promotion, including the Inter-Agency Standing Committee (IASC) Guidelines, UNICEF’s Helping Adolescent Thrive Toolkit and meta-analyses of adolescent mental health interventions (Barry et al., 2013; Das et al., 2016). This review informed the identification of core competencies and content areas. GRS then developed and refined activities through participatory design workshops with young people, Coaches, and staff in multiple countries to ensure the program’s content was engaging, culturally relevant, and feasible in low-resource settings.
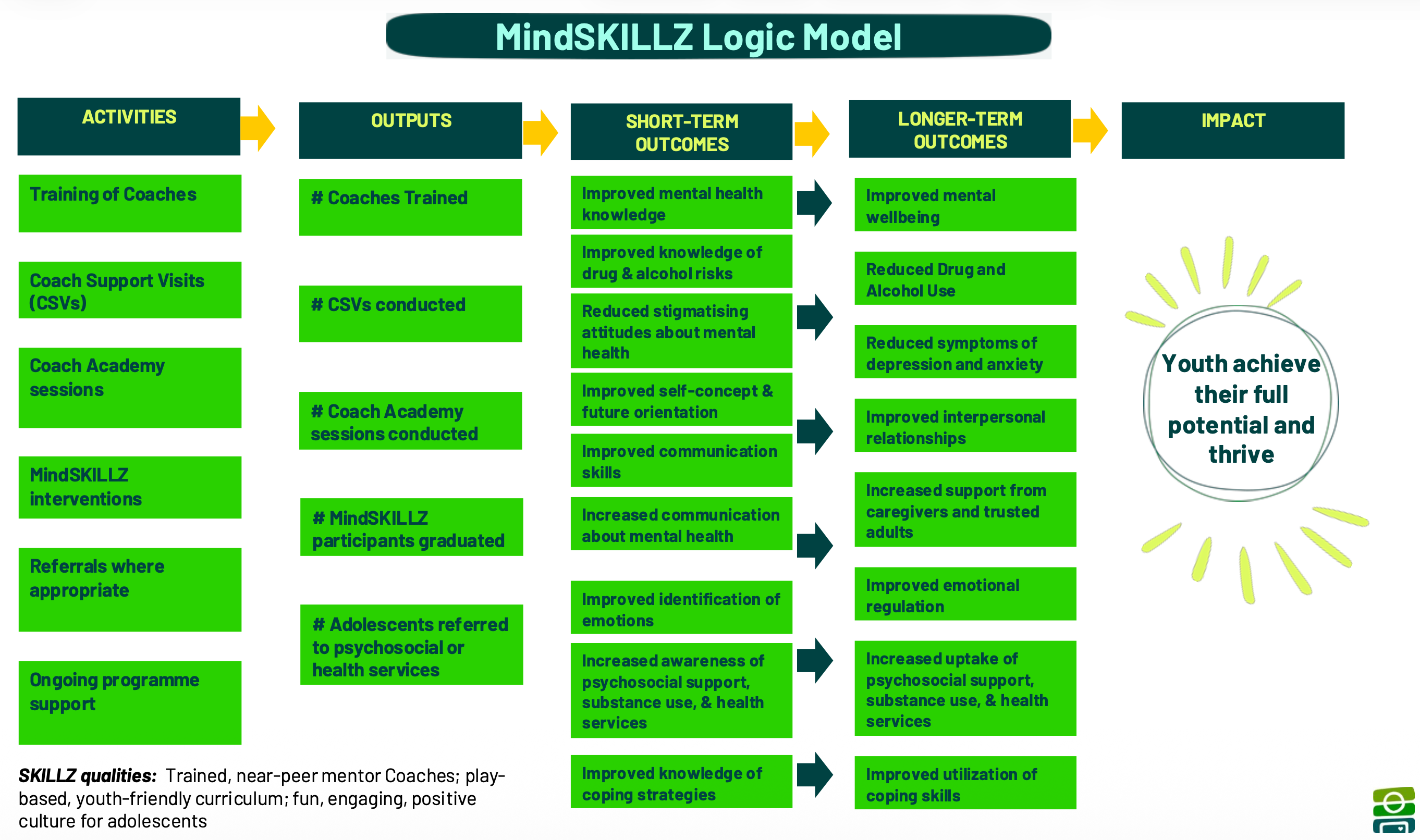
A logic model and curriculum framework were subsequently developed to articulate the program’s theory of change. Logic models clarify inputs and activities are expected to generate outputs and lead to short and long-term outcomes. Figure 1 presents the logic model for MindSKILLZ, illustrating how program activities are intended to produce outputs, short-term and longer-term outcomes, culminating in the desired impact: youth achieving their full potential and thriving.
A pre-post questionnaire aligned with the logic model was developed to assess short-term changes in mental health knowledge, attitudes, and help-seeking. Items were selected for their relevance to program content and desired outcomes, while accounting for practical constraints such as limited session time, participant attention, and administration burden. The analyses of routine monitoring data presented in this paper focuses primarily on short-term outcomes, consistent with GRS’s routine monitoring approach.
Although MindSKILLZ maintains a standardized core across countries, it is adapted through consultations with local stakeholders, including Coaches and youth. Adaptations primarily involve translation into local languages and contextualization of scenarios and role-plays. For example, role-playing activities incorporate locally relevant names and situations, transforming universal challenges, such as peer pressure, into contextually meaningful examples that enhance engagement and skill application.
Figure 1
The MindSKILLZ program is 10-12 sessions, each 45-60 minutes, hosted once or twice a week (i.e., 4-12 weeks long or 15-25 hours of contact time). Interventions are delivered in person using one of three methods: school-based, community-based, and facility-based.
School-based: School-based programs take place within educational environments, either during regular school hours or as extracurricular activities on school grounds after classes. This approach leverages the existing school infrastructure, making it easier to reach large groups of adolescents. GRS must also engage school governing bodies, principals, and teachers to get permission to deliver the program, and may benefit programs from the support of the school community.
Community-based: Community-based programs are implemented in various local settings outside of schools, such as sports fields, churches, community centers, or other gathering places. This method is designed to engage adolescents who may not be reached through schools, including those who are out of school or prefer informal environments. Community-based delivery may involve partnerships with local organizations, religious groups, or sports clubs.
Facility-based: Facility-based programs are conducted at health facilities, such as community clinics, requiring collaboration with government health departments. This method is used for GRS’s work for adolescents living with HIV, which is integrated into care and treatment services provided by local healthcare facilities, making it easier to identify and address specific needs. Facility-based delivery happens at dedicated spaces in or near the facility and is coordinated with adolescents’ access to other health service.
METHODS
Sampling and Pre-Post Questionnaire Procedures
As part of routine monitoring, GRS randomly samples approximately 20% of programs delivered for pre-post data collection. This sampling approach balances the need for outcomes monitoring with available implementation resources and staff capacity. Differences in participant numbers across countries reflect the relative scale of MindSKILLZ programming in each country during the evaluation period. Additionally, for the current analysis, the World Health Organization-5 (WHO-5) Well-Being Index (WHO, 1998) was administered to a subset of participants who received the pre/post questionnaire in Zambia and Zimbabwe. This subset of participants was selected based on program implementation schedules to allow piloting of the instrument prior to broader integration into routine monitoring systems.
In line with GRS’s organizational procedures, adolescents and their parents agreed for the adolescent to participate in the program, including the potential administration of pre-post questionnaires. Adolescents were informed that questionnaire completion was voluntary, that they could decline participation, and that they were not required to answer any specific questions.
Questionnaires are administered by Coaches immediately before and after the program, either via pen-and-paper or mobile phones. GRS uses an Android-based mobile data collection application, Comcare. This application uploads data in real time when an internet connection is available or stores it locally and syncs it to GRS’s online data management system on Salesforce when connectivity is restored. Paper-based questionnaires are entered directly into GRS’s online database or into Microsoft Excel and uploaded into the Salesforce system.
Pre-Post Questionnaire Measures
As with GRS’s other routine monitoring tools, the MindSKILLZ questionnaire included brief demographic questions (i.e., age, gender) and custom items that directly reflected program content alongside items from validated mental health scales. GRS generated 12 custom items guided by the MindSKILLZ logic model to measure the constructs of mental health knowledge, knowledge of coping skills, and self-concept. For example, the item “I know how to express my anger without being violent” was designed to align with curriculum content on anger management and emotional regulation. Additionally, GRS incorporated 13 items from the help-seeking and stigma sub-scales of the Mental Health Literacy Scale (MHLS) in the questionnaire, given their relevance to MindSKILLZ. The MHLS is a validated tool designed to assess an individual’s knowledge and understanding of mental health conditions, stigma, risk factors, and help-seeking behaviors. Evidence supports its reliability and validity across diverse populations (Topp et al., 2015; WHO, 1998).
Internal consistency of groupings of items by construct was assessed for reliability using Cronbach’s alpha (α) (Cho & Kim, 2015; Taber, 2018). Among the custom items, mental health knowledge demonstrated low reliability (α=0.47), coping skills demonstrated acceptable reliability (α=0.72), and self-concept demonstrated moderate reliability (α=0.64). The MHLS help-seeking and stigma subscales demonstrated moderate reliability (α=0.61 and α=0.67, respectively).
The WHO-5 is a five-item questionnaire that measures subjective psychological well-being over the past two weeks (WHO, 1998). Each of the five items (e.g., “I have felt calm and relaxed”) is rated on a 0 to 5 scale, where 0 indicates “at no time” and 5 indicates “all of the time.” Higher scores indicate greater well-being, with scores ≤50 points suggesting possible mental health concerns and warranting follow-up. A change in score of 10+ points indicates a clinically meaningful change. The scale has been extensively validated in clinical and non-clinical populations (Topp et al., 2015).
Expert and Youth Questionnaire Review
As part of its routine monitoring processes, GRS collects feedback on its pre-post questionnaires to improve the measurement tools. As such, a structured expert and adolescent review of the MindSKILLZ questionnaire was conducted. Five experts provided input via online surveys and interviews, exploring the questionnaire’s relevance, clarity, and alignment with program objectives. Expert contributors included: a clinical psychologist with extensive knowledge of mental health measures; a university-based implementation science researcher with a deep understanding of GRS programs; a researcher from a Kenyan youth development organization with extensive experience in pragmatic evaluations; and the Monitoring and Evaluation team at a leading youth organization with strong knowledge of multicultural mental health measures. Surveys for experts provided the pre-post questionnaire items and solicited feedback on their clarity and relevance. The surveys also requested suggestions for other relevant measures of mental health constructs and general suggestions for improving the pre-post questionnaire. Experts were asked to complete the survey and then participate in a brief 30-minute interview to expand on their feedback from the survey.
Additionally, two focus groups with youth contributors were held to obtain feedback directly from the population of interest. These focus groups, lasting approximately 60-minutes, sought to capture perspectives and experiences in a group context to ensure the pre-post questionnaire would be both developmentally appropriate and meaningful to adolescents. Youth contributors were from GRS’ Youth Advisory Committee (YAC), an internal GRS group comprised of young leaders from the communities where it works. Youth contributors also included Coaches in Zambia, who had experience delivering GRS’s mental health programs and administering pre-post questionnaires. One focus group discussion was held with 8 YAC members, and a second focus group was held with 10 GRS Coaches in Zambia. Focus groups elicited feedback on the wording of questionnaire items and how to improve both the wording and delivery processes going forward.
Data Analyses
MindSKILLZ Pre-Post Questionnaires
Pre-post questionnaire data from programs delivered in Kenya, Zambia, and Zimbabwe between January 1, 2022, and December 31, 2024, were exported from Salesforce in Microsoft Excel format and analyzed using IBM SPSS Statistics 30.0 (IBM Inc., 2024). The 12 custom items and 13 MHLS items used true/false response options, which were treated as binary variables and scored as 0 = incorrect and 1 = correct. For each participant, the mean score was calculated as the average number of correct responses across all items at each time point (pre- and post-test). Since items were coded dichotomously, the mean score represents the proportion (or percentage) of items answered correctly. First, paired t-tests were conducted to compare mean pre-and post-test scores across countries with effect sizes calculated using Cohen’s 𝑑. Paired t-tests were also used to examine item-by-item changes and change by construct grouping. Then, analyses using one-way ANOVA were performed to examine possible differences in pre-post change metrics by country, delivery method, and by gender and age.
Finally, analyses of WHO-5 data collected from a subset of MindSKILLZ program participants in Zambia and Zimbabwe were performed. Total scores ranging from 0 to 25 were converted to a 0–100-point scale by multiplying the sum by four (Topp et al., 2015). Changes in scores were examined from pre- to post-intervention. Additionally, the proportion of participants from each country who showed clinically meaningful changes (i.e., 10+ point changes) was assessed. Analyses used listwise deletion to address missing data; 6.6% of cases were excluded due to incomplete responses. For each item-level paired comparison, participants missing either a pre- or post-response for that item were excluded from that specific analysis, resulting in minor variation in sample sizes across items. Data were also checked to ensure data fell within expected ranges and values, and skewness and kurtosis values were within acceptable thresholds consistent with common guidelines for large samples.
Expert and Youth Questionnaire Review
The first author conducted a thematic analysis using an iterative, inductive approach to identify key patterns in expert and youth feedback (Braun & Clarke, 2019) on the measurement tool. Data from online surveys and focus group discussions were first reviewed for familiarization and then coded to capture recurring or important ideas related to the questionnaire’s design, clarity, and program alignment. Coded responses were grouped into overarching themes, including concerns about questionnaire length, response scale limitations, terminology, cultural relevance, and construct alignment.
Ethical considerations
The activities reported in this manuscript were conducted as part of routine monitoring of GRS programming. Because the primary purpose of these activities was to inform ongoing program delivery rather than to contribute to generalizable knowledge through systematic investigation, the institutional review board affiliated with the senior author determined that the activities described do not meet the definition of human subjects research.
RESULTS
MindSKILLZ Questionnaire Analyses
Overall Pre-Post Change
Analyses of the overall MindSKILLZ effects drew from pre-post questionnaire data collected from 2,286 program participants, with 67.9% from Kenya, 12.0% from Zambia, and 20% from Zimbabwe. Combined, the programs had a median age of 12.92 years, and the gender distribution of participants was balanced, with 52.7% identifying as female and 47.3% as male. MindSKILLZ delivery methods varied across and within countries, including community-based (48.1%), school-based (37.7%), and health facility-based programs (14.2%). A high majority (92.3%) of participants graduated from the program by attending at least 80% of the sessions.
Table 1 – MindSKILLZ Program Participant and Delivery Data by Country
| Country | N | Mean Age | Female
(%) |
Graduation
(%) |
Delivery Method (%) | ||
| Community | School | Health | |||||
| Kenya | 1,553 | 12.1 | 52.7 | 89.4 | 66.1 | 30.7 | 3.2 |
| Zambia | 275 | 16.6 | 56.2 | 98.3 | 15.7 | 84.3 | 0.0 |
| Zimbabwe | 458 | 13.4 | 50.7 | 98.9 | 0.0 | 0.0 | 100.0 |
| OVERALL | 2,286 | 12.9 | 52.7 | 92.3 | 48.1 | 37.7 | 14.2 |
Delivery Methods
Results of paired t-tests demonstrated statistically significant improvements across all countries and overall from pre- to post-test on the 25-item questionnaire (Table 2). MindSKILLZ Zimbabwe achieved the largest effect size (d=−1.393, 95% CI: −1.521,−1.264). MindSKILLZ Kenya showed the greatest percentage change (+32.9%) with a large effect size (d=−0.813, 95% CI: −0.870,−0.756). MindSKILLZ Zambia showed moderate effect sizes. Overall, there was an average pre-test score of 67.5%, increasing to 88.0% post-test (+30.5%, p<0.001), with a large effect size (d=−0.864, 95% CI: −0.912,−0.815). All effect sizes were either moderate or large, indicating meaningful improvements in pre to post-test scores.
Table 2 – Overall and Country Pre-to-Post Intervention Results for the 25-item MindSKILLZ Questionnaire
| Country | Pre-Score Mean (%) | Post-Test Mean (%) | Change % | p-value | Effect size (Cohen’s d) | 95% CI (Cohen’s d) |
| Kenya | 64.6 | 85.9 | 32.9 | <.001 | −0.813 | −0.870,−0.756 |
| Zambia | 72.8 | 84.5 | 16.2 | <.001 | −0.708 | −0.840,−0.575 |
| Zimbabwe | 73.9 | 97.3 | 31.5 | <.001 | −1.393 | −1.521,−1.264 |
| OVERALL | 67.5 | 88.0 | 30.5 | <.001 | -0.864 | -0.912, -0.815 |
Item-By-Item Changes
The percentage change from pre- to post-test for each of the 25 questionnaire items is shown in Table 3, where items 1-12 are custom GRS items, and 13-25 are taken from the MHLS. Items showing the greatest improvement were concentrated in the stigma and help-seeking domains. For example, “People with mental illness are dangerous” improved by 70.7% and “A mental illness is a sign of personal weakness” improved by 60.3%. Help-seeking items such as, “If I had a mental illness, I would not tell anyone”, also showed large improvements, while items that were already high at pre-test, such as “When I express my feelings clearly people understand me better” (80.2% pre-test), showed smaller but still meaningful gains.
Table 3 – Pre-to-Post Questionnaire Analysis for Aggregated MindSKILLZ Data
| Statement | N | Pre-Score Mean (%) | Post-Score Mean (%) | Change (%) |
| 1. When I express my feelings clearly people understand me better. | 2.279 | 80.2 | 95.9 | 19.6 |
| 2. I have skills that help me bounce back from difficult situations. | 2.281 | 69.8 | 93.7 | 34.3 |
| 3. Stress is a normal part of life. | 2.281 | 67.6 | 92.4 | 36.6 |
| 4. I can reach my goals in life. | 2.230 | 80.5 | 96.2 | 19.4 |
| 5. If I have a problem. I have someone in my life I can go to for support. | 2.280 | 77.2 | 95.1 | 23.2 |
| 6. I can identify my strengths or things that I am good at in life. | 2.277 | 74.1 | 95.2 | 28.5 |
| 7. Self-control helps you make smart decisions when you are angry or upset. | 2.278 | 74.9 | 95.3 | 27.2 |
| 8. Society expects boys and girls to deal with their emotions differently. | 2.273 | 62.2 | 88.2 | 41.8 |
| 9. I know how to express my anger without being violent. | 2.279 | 67.2 | 91.8 | 36.5 |
| 10. Listening carefully to others is an important communication skill. | 2.280 | 78.0 | 96.1 | 23.2 |
| 11. Drinking too much alcohol can have serious negative consequences for mental and physical health. | 2.278 | 74.8 | 93.9 | 25.5 |
| 12. I can understand how others are feeling and be sensitive to their emotions. | 2.279 | 69.2 | 90.2 | 30.3 |
| 13. I am confident that I know where to seek information about mental illness. | 2.281 | 62.3 | 91.4 | 46.8 |
| 14. I am confident using the computer or telephone to seek information about mental illness. | 2.279 | 59.9 | 84.2 | 40.7 |
| 15. I am confident attending face to face appointments to seek information about mental illness. | 2.276 | 61.3 | 86.6 | 41.1 |
| 16. I am confident I have access to resources that I can use to seek information about mental illness. | 2.278 | 59.7 | 86.3 | 44.6 |
| 17. People with mental illness could snap out of it if they wanted. | 2.278 | 52.3 | 52.6 | 0.6 |
| 18. A mental illness is a sign of personal weakness. | 2.280 | 48.3 | 77.5 | 60.3 |
| 19. A mental illness is not a real medical illness. | 2.278 | 57.0 | 82.7 | 45.1 |
| 20. People with mental illness are dangerous. | 2.274 | 47.4 | 80.9 | 70.7 |
| 21. It is best to avoid people with mental illness so that you don’t develop this problem. | 2.276 | 57.5 | 86.7 | 50.8 |
| 22. If I had a mental illness. I would not tell anyone. | 2.271 | 62.0 | 89.9 | 45.0 |
| 23. Seeing a mental health professional means you are not strong enough to manage your own difficulties. | 2.273 | 59.6 | 86.3 | 44.9 |
| 24. If I had a mental illness. I would not seek help from a mental health professional. | 2.276 | 65.4 | 89.7 | 37.1 |
| 25. I believe treatment for a mental illness provided by a mental health professional would not be effective. | 2.278 | 55.7 | 84.2 | 51.3 |
Note: Positive percentage changes show improvements in the intended direction. For example. more participants disagreed with harmful beliefs like “People with mental illness are dangerous.” which means stigma went down and attitudes improved.
Intentional, Person-Centred Approach
Changes by Construct Groupings
When examining changes in items grouped by mental health construct, pre-post improvements in help-seeking attitudes had the largest effect size, and a 43.6% increase. The greatest pre-post percentage change improvement occurred in reducing mental health stigma, which increased by 44.8% (Table 4). Mental health knowledge improved by 34.2%, while self-concept and future orientation increased by 27.3%. Knowledge of coping strategies and interpersonal skills showed a 26.3% increase.
Table 4 – Pre- and Post-Intervention Results by Mental Health Constructs for Aggregated MindSKILLZ data
| Mental health construct | N | Pre-score mean (%) | Post -Score mean (%) | Change (%) | p-value | Effect size (Cohen’s d) | 95% CI (Cohen’s d) |
| Knowledge of coping/interpersonal skills | 2,258 | 74.5 | 94.0 | 26.3 | <.001 | -0.656 | -0.701,
-0.610 |
| Positive self-concept and future orientation | 2,220 | 74.6 | 95.0 | 27.3 | <.001 | -0.594 | -0.639, -0.548 |
| Mental health knowledge | 2,265 | 68.2 | 91.5 | 34.2 | <.001 | -0.647 | -0.692, -0.601 |
| Mental health stigma | 2,243 | 55.0 | 79.6 | 44.8 | <.001 | -0.707 | -0.753, -0.661 |
| Help-seeking attitudes | 2,251 | 60.6 | 87.1 | 43.6 | <.001 | -0.787 | -0.834 -0.740 |
Changes by Country and Participant Characteristics
A one-way ANOVA revealed a statistically significant difference in pre-post changes across the three country programs (p < 0.001). Specifically, MindSKILLZ Zimbabwe (change in pre-post mean score = +5.83) and MindSKILLZ Kenya (change in pre-post mean score = +5.32) achieved significantly larger pre-post changes than MindSKILLZ Zambia (change in pre-post mean score = +2.90; p < 0.001). However, the effect size was small (η² = 0.020). No significant difference was found between MindSKILLZ Zimbabwe and MindSKILLZ Kenya.
Analyses examining differences in pre–post questionnaire results by gender, age, and delivery method revealed minimal practical differences. Gender was not associated with meaningful differences in change scores; independent samples t-tests showed no significant differences between males and females across programs (p > 0.05). Age was a statistically significant predictor of pre–post score changes (p < 0.001), but the effect was small (β = -0.122), indicating only a weak negative relationship, with younger participants experiencing slightly greater improvements. For example, participants aged 10–14 showed the largest mean improvement (33.1%), compared to 20.0% for those aged 15–19 and 13.8% for those aged 20+, with statistically significant differences between the 10–14 and 15–19 groups (mean difference = 1.72, p < 0.001) and between the 10–14 and 20+ groups (mean difference = 2.90, p = 0.004). Delivery method also had a statistically significant effect in MindSKILLZ Kenya, with community-based sessions outperforming health facility and school-based delivery (F = 10.198, p < 0.001), though the effect size was very small (η² ≈ 0.010).
WHO-5 Well-Being Index Analyses
The WHO-5 wellbeing index was completed by 791 participants in Zambia and 951 participants in Zimbabwe (n=1,742 in total). Participants were 60% and 54% female in Zambia and Zimbabwe, respectively, with mean ages of 16.1 years (SD=3.3) and 13.6 years SD=2.3). The average change in score in Zimbabwe was clinically significant (i.e., a 10+ point change) overall with a 16 point increase. The average change in Zambia did not reach clinical significance but showed a 6 point increase. A significant improvement in well-being (i.e., a 10+ point increase) was also observed in 42% of participants in Zambia and 65% in Zimbabwe. The percentage of participants scoring ≤50 (i.e., having poor mental health and possible depression) decreased notably in both settings. In Zambia, the proportion dropped from 21% at baseline to 15% post-program, while in Zimbabwe, it declined from 6% to 1%.
Expert and Youth Questionnaire Review
Experts and youth commended the MindSKILLZ questionnaire for effectively addressing adolescent mental health challenges in a simple, developmentally appropriate manner. Experts explained that the MindSKILLZ questionnaires “comprehensively measure the emotional, social, and mental health status of young people” and “include clear and straightforward statements covering a broad range of mental health constructs.” Youth reviewers also praised the tool for its contextual relevance. A GRS Coach in Zambia said, “The statements are related to things [participants] go through in the community.” However, the focus of the expert and youth review was to identify areas for improvement in the questionnaire, and five main themes were identified.
Concerns About Questionnaire Length
Experts and youth noted that the questionnaire was sometimes too long, potentially leading to participant fatigue. Several recommended reducing it to 15–20 items. A GRS Coach in Zambia observed, “At times, I think participants just circle because the questionnaire is long, and they just wanted to finish.” YAC members from the youth focus group echoed this concern, recommending a maximum of 20 items to sustain adolescent attention and reduce the risk of careless responding.
Response Scale Limitations
Experts recommended expanding response options to capture more nuanced answers. One external expert suggested, “You would get a more sensitive response if you offered more options (e.g., a 7-point scale would be more common). Few of us are 100% yes or no for most issues.” YAC members also raised concerns about response patterns, noting that most questionnaire items were worded so that “agree” was the expected correct answer, which could lead participants to respond in socially desirable ways. They suggested alternating the wording of items so that agreement and disagreement were both represented across the questionnaire.
Terminology
Simplifying wording was highlighted as essential to ensure participant comprehension. Coaches reported that participants often struggled with terms such as “vigorous,” “snap out of it,” “bounce back,” “just mad,” and “self-control.” External experts additionally noted inconsistent use of mental health terminology across items. For example, using “mental illness” and “mental health challenge” interchangeably, and recommended standardizing language to minimise confusion.
Cultural Relevance
Youth emphasized the importance of incorporating contextually relevant topics, particularly Sexual and Reproductive Health and Rights (SRHR). A YAC member from Zimbabwe noted, “Teenage pregnancy and early marriages, these topics are supposed to be discussed especially in rural areas where cases of teen pregnancy and early marriages are high.” YAC members further explained that SRHR issues directly affect adolescents’ mental health in the communities where GRS works, and recommended that the questionnaire consider how such stressors are experienced by young people. External experts complemented this perspective by recommending the inclusion of items addressing other contextually salient topics such as peer pressure, academic stress, sleep quality, and experiences of social support, arguing that these domains are both relevant to adolescent mental health and underrepresented in the current tool.
Construct Alignment
Experts recommended ensuring that the pre–post questionnaire aligns with the MindSKILLZ logic model and clearly reflects the mental health constructs being measured. They observed a gap between session objectives and what the questionnaire currently assesses. One external expert noted that while program sessions focus on goal-setting, coping skills, help-seeking, and emotional resilience, few questionnaire items directly assess these constructs, and suggested organizing items explicitly by mental health construct to improve transparency and interpretability. Another expert flagged specific item-level concerns, including that some items may not be directly related to mental health (e.g., an item on goal achievement).
DISCUSSION
This paper presented an analysis of routine monitoring data from GRS’s MindSKILLZ mental health program across three African countries. We proceed to discuss our findings and their implications within the context of Aim 1 (i.e., MindSKILLZ questionnaire analyses) and Aim 2 (i.e., expert and youth questionnaire review). These considerations inform how improvements observed in routine data should be interpreted for program refinement, scale-up, and future evaluation design.
MindSKILLZ Questionnaire Results and Implications
The observed pre-to-post-program improvements suggest meaningful gains in adolescent mental health promotion across multiple domains. In particular, the improvement in help-seeking attitudes, which demonstrated a large effect size, directly reflects program goals to strengthen adolescents’ sense of agency and access to care. Similarly, reductions in mental health stigma, which also yielded large effects, represent an important outcome given that stigma is a well-documented barrier to help-seeking and social support in the program settings (Gulliver et al., 2010). Smaller, though still notable, improvements in mental health knowledge, self-concept, and coping and interpersonal skills represent foundational components of adaptive help-seeking and coping behaviors (Gulliver et al., 2010) and have been linked to improved mental health outcomes among adolescents (Skeen et al., 2019).
Pre-post gains were observed across countries, delivery methods, and participant groups, highlighting the program’s flexibility and broad appeal. Still, differences by country, and, to a lesser extent, delivery method and age, suggest that the implementation setting may have shaped outcomes even when core elements were constant. This is consistent with insights from the field of implementation science that effective scale-up depends on specifying and delivering core components with fidelity while allowing nonessential features to adapt to local conditions (Aarons et al., 2011; Meyers et al., 2012). GRS’s routine monitoring and analyses are not equipped to identify which implementation determinants (e.g., coach competency, school/community/facility buy-in, or curriculum fidelity) most drove variation. GRS’s routine monitoring systems also do not measure implementation outcomes, such as acceptability, appropriateness, and feasibility (Proctor et al., 2011). Deeper exploration of implementation determinants and outcomes should be pursued in research studies of MindSKILLZ programming.
Beyond these differences, the most notable trend was greater improvement among participants aged 10–14 years relative to older groups. Based on this finding, GRS decided to recommend prioritizing MindSKILLZ for ages 10–14 while also providing guidance for age-appropriate adaptations for older adolescents, including deeper discussion prompts, more technical mental health content, and scenarios tailored to their experiences.
WHO-5 results indicate trends towards improved emotional and psychological well-being. The overall changes in Zimbabwe met clinically meaningful thresholds per WHO scoring guidelines. These signals align with MindSKILLZ’s goals and suggest that a non-clinical, scalable, SFD platform may support clinically relevant improvements in mental health and well-being. Moreover, decreases across both countries in the portion of participants scoring in the “poor well-being” range (≤50 points) suggest potential benefits for adolescents starting with psychological distress or low well-being, as well as for the broader adolescent populations. Future implementation should prioritize access for underserved adolescents exposed to mental health risk factors, such as out-of-school youth and those in humanitarian settings.
Pre-Post Questionnaire Refinement
The mental health knowledge construct demonstrated low internal consistency (α = 0.47), which reflects program alignment rather than a validated psychometric scale. Items were developed to correspond directly to program content and curriculum objectives, prioritizing face validity and program relevance. While this limits interpretive precision at the construct level, item-level findings remain informative for practitioners seeking to understand which specific content areas showed the greatest change.
While routine data collection provides valuable insights, measuring mental health promotion outcomes among young people presents unique challenges (Hunter et al., 1996; Kwan & Rickwood, 2015). Validated external measures improve reliability, but tools must also be practical for implementation. Striking a balance between standardization and real-world feasibility is essential.
Based on expert and youth feedback, GRS made several refinements to the MindSKILLZ questionnaire. First, the review process highlighted the need to simplify questionnaire language, particularly in items drawn from the MHLS and WHO-5 Well-Being Index. Terms such as “vigorous,” “snap out of it,” and “self-control” were found to be difficult for younger participants to understand. The revised pre-post questionnaire now features clearer terminology, improved phrasing, and standardized mental health language to improve comprehension.
Second, the analysis highlighted the importance of strengthening routine program monitoring through qualitative data collection. Incorporating structured qualitative and observational assessments alongside quantitative measures would provide a more comprehensive understanding of program effects. In response, GRS is developing and piloting standardized approaches for routinely collecting qualitative data to complement pre–post questionnaire findings.
Finally, GRS refined its use of standardized measures. The WHO-5, which provides a brief and accessible assessment of well-being, will now be implemented across all relevant programs. Additionally, several confusing MHLS items related to confidence in seeking information were removed to improve the questionnaire’s clarity and usability.
Limitations
This analysis is limited by its reliance on routine program monitoring data rather than data collected through a prospective human subjects research study. As such, we cannot draw conclusions about effectiveness, causality, or long-term outcomes. Routine data collection is also subject to variability in administration, biases, and participant comprehension. Expert and youth feedback was limited to a small sample.
CONCLUSION
Routine monitoring of GRS’s MindSKILLZ program shows consistent pre–post gains in mental health knowledge, reduced stigma, stronger help‐seeking attitudes, and improved psychological well‐being across real-world, low-resource settings. These findings are informing program refinements, including prioritizing access for younger, underserved, and structurally marginalized adolescents; making age-appropriate adaptations; simplifying and clarifying pre–post tools aligned with core constructs; and promoting more systematic use of the WHO‑5. Still, rigorous research is needed to establish the causal impact of MindSKILLZ on mental health outcomes. Cross-country comparative analyses provide insights into how context shapes program implementation and outcomes, guiding adaptive strategies for scaling SFD and mental health programs in diverse settings. More broadly, organizations implementing similar programs should consider how routine monitoring data can drive continuous improvement and contribute to the evidence base for adolescent mental health promotion in SSA.
CONFLICTS OF INTEREST
The authors have no conflicts of interest to disclose.
FUNDING
This work was supported by the generous support of the Stavros Niarchos Foundation, the Vitol Foundation, the MAC AIDS Fund, and the Oak Foundation.
ACKNOWLEDGEMENTS
We gratefully acknowledge the young people, coaches, staff, communities, and partners who make Grassroot Soccer’s mental health programs possible. Their commitment, insight, and everyday efforts are the foundation of this work.
REFERENCES
Aarons, G. A., Hurlburt, M., & Horwitz, S. M. (2011). Advancing a conceptual model of evidence-based practice implementation in public service sectors. Administration and Policy in Mental Health, 38(1), 4–23. https://doi.org/10.1007/s10488-010-0327-7
Bandura, A. (1977). Self-efficacy: Toward a unifying theory of behavioral change. Psychological Review, 84(2), 191–215. https://doi.org/10.1037/0033-295X.84.2.191
Bandura, A. (1986). Social Foundations of Thought and Action: A Social Cognitive Theory. Prentise Hall.
Barkley, C. K., Nyakonda, C. N., Kuthyola, K., Ndlovu, P., Lee, D., Dallos, A., Kofi-Armah, D., Obeng, P., & Merrill, K. G. (2025). A gamified digital mental health intervention across six Sub-Saharan African countries: A cross-sectional evaluation of a large-scale implementation. International Journal of Environmental Research and Public Health, 22(8), 1281. https://doi.org/10.3390/ijerph22081281
Barry, M. M., Clarke, A. M., Jenkins, R., & Patel, V. (2013). A systematic review of the effectiveness of mental health promotion interventions for young people in low and middle income countries. BMC Public Health, 13(1), 835. https://doi.org/10.1186/1471-2458-13-835
Berkel, C., Gallo, C. G., Sandler, I. N., Mauricio, A. M., Smith, J. D., & Brown, C. H. (2019). Redesigning implementation measurement for monitoring and quality improvement in community delivery settings. The Journal of Primary Prevention, 40(1), 111–127. https://doi.org/10.1007/s10935-018-00534-z
Braun, V., & Clarke, V. (2019). Reflecting on reflexive thematic analysis. Qualitative Research in Sport, Exercise and Health, 11(4), 589–597. https://doi.org/10.1080/2159676X.2019.1628806
Centre for Effective Services. (2022). Monitoring and Evaluation | Implementation. CES guide to implementation. https://implementation.effectiveservices.org/enablers/monitoring-and-evaluation
Chibanda, D., Mesu, P., Kajawu, L., Cowan, F., Araya, R., & Abas, M. A. (2011). Problem-solving therapy for depression and common mental disorders in Zimbabwe: Piloting a task-shifting primary mental health care intervention in a population with a high prevalence of people living with HIV. BMC Public Health, 11(1), 828. https://doi.org/10.1186/1471-2458-11-828
Cho, E., & Kim, S. (2015). Cronbach’s Coefficient Alpha: Well known but poorly understood. Organizational Research Methods, 18(2), 207–230. https://doi.org/10.1177/1094428114555994
Clark, T. S., Friedrich, G. K., Ndlovu, M., Neilands, T. B., & McFarland, W. (2006). An adolescent-targeted HIV prevention project using African professional soccer players as role models and educators in Bulawayo, Zimbabwe.Aids and Behavior, 10(Journal Article), S77–S83. https://doi.org/10.1007/s10461-006-9140-4
Coakley, J. (2011). Youth sports: What counts as “positive development?” Journal of Sport & Social Issues, 35(3), 306–324. https://doi.org/10.1177/0193723511417311
Coalter, F. (2013). Sport for Development: What Game Are We Playing? Routledge.
Das, J. K., Salam, R. A., Lassi, Z. S., Khan, M. N., Mahmood, W., Patel, V., & Bhutta, Z. A. (2016). Interventions for adolescent mental health: An overview of systematic reviews. The Journal of Adolescent Health, 59(Suppl. 4), S49–S60. https://doi.org/10.1016/j.jadohealth.2016.06.020
Das-Munshi, J., Lund, C., Mathews, C., Clark, C., Rothon, C., & Stansfeld, S. (2016). Mental health inequalities in adolescents growing up in Post-Apartheid South Africa: Cross-sectional survey, SHaW Study. PLOS ONE, 11(5), Article e0154478. https://doi.org/10.1371/journal.pone.0154478
Doyle, A. M., Bandason, T., Dauya, E., McHugh, G., Grundy, C., Simms, V., Chibanda, D., & Ferrand, R. (2023). Common mental health and emotional and behavioural disorders among adolescents and young adults in Harare and Mashonaland East, Zimbabwe: A population-based prevalence study. BMJ Open, 13(3), Article e065276. https://doi.org/10.1136/bmjopen-2022-065276
Eather, N., Wade, L., Pankowiak, A., & Eime, R. (2023). The impact of sports participation on mental health and social outcomes in adults: A systematic review and the ‘Mental Health through Sport’ conceptual model. Systematic Reviews, 12, 102. https://doi.org/10.1186/s13643-023-02264-8
Fusar-Poli, P. (2019). Integrated mental health services for the developmental period (0 to 25 Years): A critical review of the evidence. Frontiers in Psychiatry, 10. https://www.frontiersin.org/articles/10.3389/fpsyt.2019.00355
Gulliver, A., Griffiths, K. M., & Christensen, H. (2010). Perceived barriers and facilitators to mental health help-seeking in young people: A systematic review. BMC Psychiatry, 10, 113–121. https://doi.org/10.1186/1471-244X-10-113
Hansell, A. H., Giacobbi, P. R., & Voelker, D. K. (2021). A scoping review of sport-based health promotion interventions with youth in Africa. Health Promotion Practice, 22(1), 31–40. https://doi.org/10.1177/1524839920914916
Hart, C., & and Norris, S. A. (2024). Adolescent mental health in sub-Saharan Africa: Crisis? What crisis? Solution? What solution? Global Health Action, 17(1), Article 2437883. https://doi.org/10.1080/16549716.2024.2437883
Hunter, J., Higginson, I., & Garralda, E. (1996). Systematic literature review: Outcome measures for child and adolescent mental health services. Journal of Public Health, 18(2), 197–206. https://doi.org/10.1093/oxfordjournals.pubmed.a024480
IBM Inc., (2024). IBM SPSS Statistics (Version 30.0.0) [macOS]. IBM Corporation.
Jörns-Presentati, A., Napp, A.-K., Dessauvagie, A. S., Stein, D. J., Jonker, D., Breet, E., Charles, W., Swart, R. L., Lahti, M., Suliman, S., Jansen, R., Heuvel, L. L. van den, Seedat, S., & Groen, G. (2021). The prevalence of mental health problems in sub-Saharan adolescents: A systematic review. PLOS ONE, 16(5), Article e0251689. https://doi.org/10.1371/journal.pone.0251689
Kaufman, Z. A., Welsch, R. L., Erickson, J. D., Craig, S., Adams, L. V., & Ross, D. A. (2012). Effectiveness of a sports-based HIV prevention intervention in the Dominican Republic: A quasi-experimental study. Aids Care-Psychological and Socio-Medical Aspects of Aids/Hiv, 24(3), 377–385. https://doi.org/10.1080/09540121.2011.608789
Kessler, R. C., Berglund, P., Demler, O., Jin, R., Merikangas, K. R., & Walters, E. E. (2005). Lifetime prevalence and age-of-onset distributions of DSM-IV disorders in the National Comorbidity Survey Replication. Archives of General Psychiatry, 62(6), 593–602. https://doi.org/10.1001/archpsyc.62.6.593
Kwan, B., & Rickwood, D. J. (2015). A systematic review of mental health outcome measures for young people aged 12 to 25 years. BMC Psychiatry, 15, 279. https://doi.org/10.1186/s12888-015-0664-x
Latimer, K., Larok, R., Nyeko, J. P., Murungi, L., Luwangula, R., Lukungu, B., Carrin, J., Nannungi, R., Comboni, D. O., Kalule, E. N., Rosenbaum, S., & Vancampfort, D. (2025). A sport-for-protection program reduces anxiety and depression in youth affected by displacement: A randomized controlled trial of the Game Connect program in Uganda. Journal of Affective Disorders, 376, 84–91. https://doi.org/10.1016/j.jad.2025.02.001
Lee, D. E. Z., Nkosi, Z., Nyakonda, C. N., Barkley, C., Dallos, A., Merrill, K. G., & Malotana, M. (2025). Lessons learnt from integrating mental health into sport-based adolescent sexual and reproductive health programmes in South Africa. South African Health Review, 27, 163–174. https://doi.org/10.61473/001c.141588
Longwe, B., Hachilensa, L., Chunga, C., Banda, K., Ng’andu, M., Shakwelele, H., Mwamba, T., Maambo, N., Michelo, J., Haimbe, P., & Mweemba, M. (2025). The Nexus of HIV, substance abuse, and mental health among adolescents in Zambia (2021–2023). Journal of Public Health in Africa, 16(1), 1229. https://doi.org/10.4102/jphia.v16i1.1229
Lubans, D., Richards, J., Hillman, C., Faulkner, G., Beauchamp, M., Nilsson, M., Kelly, P., Smith, J., Raine, L., & Biddle, S. (2016). Physical activity for cognitive and mental health in youth: A systematic review of mechanisms. Pediatrics, 138(3), Article e20161642. https://doi.org/10.1542/peds.2016-1642
Mabrouk, A., Mbithi, G., Chongwo, E., Too, E., Sarki, A., Namuguzi, M., Atukwatse, J., Ssewanyana, D., & Abubakar, A. (2022). Mental health interventions for adolescents in sub-Saharan Africa: A scoping review. Frontiers in Psychiatry, 13. https://www.frontiersin.org/articles/10.3389/fpsyt.2022.937723
McGorry, P., & Mei, C. (2023). Youth mental health: A rising public health challenge. Australasian Psychiatry, 31(3), 245–246. https://doi.org/10.1177/10398562231177350
Meffert, S. M., Lawhorn, C., Ongeri, L., Bukusi, E., Campbell, H. R., Goosby, E., Bertozzi, S. M., & Kahonge, S. N. (2021). Scaling up public mental health care in Sub-Saharan Africa: Insights from infectious disease. Cambridge Prisms: Global Mental Health, 8, Article e41. https://doi.org/10.1017/gmh.2021.41
Merrill, K. G., Merrill, J. C., Hershow, R. B., Barkley, C., Rakosa, B., DeCelles, J., & Harrison, A. (2018). Linking at-risk South African girls to sexual violence and reproductive health services: A mixed-methods assessment of a soccer-based HIV prevention program and pilot SMS campaign. Evaluation and Program Planning, 70, 12–24. https://doi.org/10.1016/j.evalprogplan.2018.04.010
Meyers, D. C., Durlak, J. A., & Wandersman, A. (2012). The quality implementation framework: A synthesis of critical steps in the implementation process. American Journal of Community Psychology, 50(3–4), 462–480. https://doi.org/10.1007/s10464-012-9522-x
Proctor, E., Silmere, H., Raghavan, R., Hovmand, P., Aarons, G., Bunger, A., Griffey, R., & Hensley, M. (2011). Outcomes for implementation research: Conceptual distinctions, measurement challenges, and research agenda. Administration and Policy in Mental Health, 38(2), 65–76. https://doi.org/10.1007/s10488-010-0319-7
Richards, J., Foster, C., Townsend, N., & Bauman, A. (2014). Physical fitness and mental health impact of a sport-for-development intervention in a post-conflict setting: Randomised controlled trial nested within an observational study of adolescents in Gulu, Uganda. BMC Public Health, 14(1), 619. https://doi.org/10.1186/1471-2458-14-619
Rotheram-Borus, M. J., Tomlinson, M., Durkin, A., Baird, K., DeCelles, J., & Swendeman, D. (2016). Feasibility of using soccer and job training to prevent drug abuse and HIV. AIDS and Behavior, 20(9), 1841–1850. https://doi.org/10.1007/s10461-015-1262-0
Schulenkorf, N., Sherry, E., & Rowe, K. (2016). Sport for Development: An Integrated Literature Review. https://doi.org/10.1123/jsm.2014-0263
Sensoy Bahar, O., Byansi, W., Nabayinda, J., Kiyingi, J., Namatovu, P., Embaye, F., McKay, M. M., Hoagwood, K., & Ssewamala, F. M. (2023). “I decided to participate….because I saw it as benefiting our community and families”: A qualitative study of lay providers’ experiences with delivering an evidence-based mental health intervention for families in Uganda. International Journal of Mental Health Systems, 17(1), 24. https://doi.org/10.1186/s13033-023-00593-8
Skeen, S., Laurenzi, C. A., Gordon, S. L., du Toit, S., Tomlinson, M., Dua, T., Fleischmann, A., Kohl, K., Ross, D., Servili, C., Brand, A. S., Dowdall, N., Lund, C., van der Westhuizen, C., Carvajal-Aguirre, L., Eriksson de Carvalho, C., & Melendez-Torres, G. J. (2019). Adolescent mental health program components and behavior risk reduction: A meta-analysis. Pediatrics, 144(2), Article e20183488. https://doi.org/10.1542/peds.2018-3488
Solmi, M., Radua, J., Olivola, M., Croce, E., Soardo, L., Salazar de Pablo, G., Il Shin, J., Kirkbride, J. B., Jones, P., Kim, J. H., Kim, J. Y., Carvalho, A. F., Seeman, M. V., Correll, C. U., & Fusar-Poli, P. (2022). Age at onset of mental disorders worldwide: Large-scale meta-analysis of 192 epidemiological studies. Molecular Psychiatry, 27(1), 281–295. https://doi.org/10.1038/s41380-021-01161-7
Taber, K. S. (2018). The use of Cronbach’s Alpha when developing and reporting research instruments in science education. Research in Science Education, 48(6), 1273–1296. https://doi.org/10.1007/s11165-016-9602-2
Topp, C., Østergaard, S., Søndergaard, S., & Bech, P. (2015). The WHO-5 Well-Being Index: A systematic review of the literature. Psychotherapy and Psychosomatics, 84, 167–176. https://doi.org/10.1159/000376585
Uhlhaas, P. J., Davey, C. G., Mehta, U. M., Shah, J., Torous, J., Allen, N. B., Avenevoli, S., Bella-Awusah, T., Chanen, A., Chen, E. Y. H., Correll, C. U., Do, K. Q., Fisher, H. L., Frangou, S., Hickie, I. B., Keshavan, M. S., Konrad, K., Lee, F. S., Liu, C. H., … Wood, S. J. (2023). Towards a youth mental health paradigm: A perspective and roadmap. Molecular Psychiatry, 28(8), 3171–3181. https://doi.org/10.1038/s41380-023-02202-z
UNDP Evaluation Office. (2002). Handbook on Monitoring and Evaluation for Results. UNDP. https://focusintl.com/RBM017-Handbook_monitoring_evaluation_for_results.pdf
WHO. (1998). Wellbeing measures in primary health care/the DEPCARE project. WHO.
Yatham, S., Sivathasan, S., Yoon, R., da Silva, T. L., & Ravindran, A. V. (2018). Depression, anxiety, and post-traumatic stress disorder among youth in low and middle income countries: A review of prevalence and treatment interventions. Asian Journal of Psychiatry, 38, 78–91. https://doi.org/10.1016/j.ajp.2017.10.029
