Francis Barchi1, Millan A. AbiNader2, Samantha C. Winter3, Lena M. Obara1, Daniel Mbogo4, Bendettah M. Thomas5, & Brittany Ammerman6
1 Rutgers, The State University of New Jersey, USA
2 University of Pennsylvania, USA
3 Columbia University, USA
4 Village Voices, Kenya
5 Nikumbuke Project, Kenya
6 Hospital for Special Surgery, USA
Citation:
Barchi, F., AbiNader, M.A., Winter, S.C., Obara, L.M., Mbogo, D., Thomas, B.M., & Ammerman, B. (2022). Improving adult women’s emotional health in rural Kenya through community soccer and the role of social support: A mixed-methods analysis. Journal of Sport for Development. Retrieved from https://jsfd.org/
ABSTRACT
This study examines the contribution of a recreational adult women’s soccer league in rural Kenya to the development goals of enhancing social support, building community cohesion, and improving women’s emotional health. Using a sequential explanatory mixed methods approach, 702 members of a women’s health and literacy program, 229 of whom played in the program’s soccer league, completed surveys about various aspects of their lives. A five-item scale, perceived support from friends (PSF), queried women’s access to emotional and instrumental support; an exploratory factor analysis confirmed this scale’s suitability as a single measure. Bivariate and multivariate analyses examined attributes associated with PSF. Based on these findings, a purposive sample of 229 soccer league members participated in focus group discussions. Women’s perceptions were examined using thematic analysis. Quantitative findings indicated that soccer league members had greater odds of reporting high social support than their non-soccer-playing peers. Qualitative findings from the final analysis sample of 201 women suggested that soccer provided a social space in which team members formed a network of friendships within and across villages, providing emotional and instrumental support they associated with decreased stress and improved well-being. Given the positive effects of soccer on adult women’s lives, similar programs, particularly in rural settings with limited resources, should be considered as development strategies.
IMPROVING ADULT WOMEN’S EMOTIONAL HEALTH IN RURAL KENYA THROUGH COMMUNITY SOCCER AND THE ROLE OF SOCIAL SUPPORT: A MIXED-METHODS ANALYSIS
Sport-for-development theory suggests that sports are an effective international development tool that improves public health, enhances socialization, promotes inclusion of those who are disadvantaged, and contributes to the economic development of communities (Lyras & Welty Peachey, 2011). Social change theories suggest that participation in sports stimulates change at the individual, cultural, and societal levels—empowering otherwise marginalized, at risk-youth, promoting gender equity, giving women voice, and empowering women to assume a greater role in the home, community, and political economy (Hancock et al., 2013; Huggins & Randell, 2007; Lyras & Hums, 2009; Meier, 2000; Ottesen et al., 2010). The notion of “football for good” is reflected in such global sports initiatives as streetfootballworld (https://www.streetfootballworld.org), WomenWin (https://www.womenwin.org) and FFA Global (https://www.ffaglobal.org) which empower young people through soccer’s capacity to foster inclusion and enhance self-efficacy.
Research on sport-for-development programming for women and girls in Sub-Saharan Africa has largely focused on youth programs (Akindes & Kirwin, 2009; Jeanes, 2013; Richards & Foster, 2013). Several sports programs for adolescent girls in Kenya have shown that team sports can have psychosocial benefits, offering both safe places in which girls can build greater confidence and self-efficacy as well as social spaces in which to form friendships and social networks (Brady, 2005; Brady & Khan, 2002; Forde, 2009; Uweza Foundation, n.d.). Although these studies provide an evidence base to support sport-for-development initiatives, recreational team sports have yet to be adopted in the region as a strategy to improve the lives of adult women, particularly those living in rural communities. The establishment of a community soccer league for adult women by the Nikumbuke Project in southeastern Kenya in 2014 provided a unique opportunity to carry out empirical research on the value of such initiatives as social development strategies, and is the focus of the current study. Our interest in the present study was to examine the ways in which the league has contributed to the Nikumbuke Project’s development goals of enhancing women’s sense of social support, building community cohesion, and improving women’s emotional health and sense of well-being.
Social Support and Emotional Health
Social support, one’s perception of belonging to a mutually beneficial network of people in which one is cared about and valued, is widely recognized as a social determinant of health, and is linked to numerous positive mental and physical health effects in studies across populations and disease conditions (Berkman & Glass, 2000; Harandi et al., 2017; Taylor, 2011; Wang et al., 2018; WHO, 2003). Social support has been found to be positively associated with emotional well-being and quality of life in various populations, including adolescents (Noret et al., 2020; Weber et al., 2010), persons living with HIV (Chandran et al., 2019; McDowell & Serovich, 2007); and caregivers (del-Pino-Casado, 2018; Ong et al., 2018). In Sub-Saharan Africa, scholars have found social support to be a significant factor in predicting depression (Breet et al., 2014; Osborn et al., 2020) and emotional well-being (Gyasi, 2019). Social support has been shown to have a moderating effect on the relationship between mental health and food insecurity (Na, 2018; Tsai, 2016) and to promote psychological resilience and reduce depression in HIV-positive populations (Kalomo, 2018; Machisa, 2018).
Social support has been identified as both a correlate and a causal contributor to well-being (Cobb, 1976; Cohen & Syme, 1985). A number of different perspectives on the pathways linking social support and health have been suggested by scholars (Lakey & Cohen, 2000). The access to emotional and instrumental support may influence health indirectly by reducing causes of stress or by motivating individuals to adopt healthier behaviors (Bloom, 1990). Other scholars suggest that social support may exert a direct effect on physiological processes, increasing an individual’s ability to fend off disease (Berkman & Glass, 2000; Uchino, 2006). Of particular relevance to the current research is the Stress and Coping Perspective, which posits that the supportive actions of others, and beliefs in the availability of such support when needed, can themselves reduce the effects of stressful events on health (Lazarus, 1966). This may be the direct result of one’s perception that he or she has access to interpersonal resources should a stressful event occur or the buffering effects of social support on the level of stress that an event can cause (Cohen & Wills, 1985). This buffering effect has been found to be most effective at reducing stress when one shares a social identity with the source of the social support (Frisch et al., 2014; McKimmie et al., 2020).
Study Aims
Previously published work by the authors reported that adult women’s participation in the league was associated with reduced experiences of physical violence and positive self-reported health status (Barchi et al., 2021, 2022). Women credited soccer with less pain, reduced worry, and greater strength and energy. Although some of these outcomes may have been the result of increased aerobic exercise, the considerable body of literature linking sports and social support suggests that the social aspects of the league, both at the team- and community- levels, may have contributed to women’s improved sense of well-being, and therefore warranted further examination. We hypothesized that: (a) women who participate in the soccer league would have greater perceived social support from friends than their peers who do not, (b) the social nature of a team sport would contribute to self-reported lower stress and improved well-being, and (c) that the adult women’s soccer league was a valuable social development tool in this setting.
METHODS
The study used a sequential explanatory mixed methods approach (Creswell & Creswell, 2017) to assess levels of perceived social support from friends among women in southeastern rural Kenya and to gain an understanding of the ways in which participation in an adult women’s soccer league may enhance social support, reduce stress, and improve well-being in this setting. An extensive literature supports the use of mixed methods in instances in which neither quantitative nor qualitative methods alone may adequately capture the trends and details of particular phenomena (e.g., Ivankova et al., 2006; Johnson et al., 2007). The sequential explanatory mixed methods approach used in this study was quantitative-dominant, enabling the study team to use quantitative methods to assess levels of social support among community members and identify significant correlates before specifying the sample and the research questions to be used in the follow-on qualitative phase (see Figure 1). Sport-for-development and social cognitive theories relating to social support provided the conceptual framework for the development of questions in both phases of the study and in the interpretation of findings. Final survey and focus group script content was further guided by the prior field experience of the research team, which included Kenyan nationals with research experience in this setting, researchers with expertise in qualitative methods, and individuals with direct involvement in the formation of the soccer league. The study was reviewed and approved by the Institutional Review Board at Rutgers University and by the National Commission for Science, Technology, and Innovation (NACOSTI) in Nairobi, Kenya.
Figure 1 – The sequential explanatory mixed methods approach

Setting
The study took place in 2018-2019 in Lunga Lunga, a sub-county of Kwale County in the Coast Region of southeastern Kenya. Located on the border with Tanzania, the sub-county is semi-arid, susceptible to extreme drought and flooding, and characterized by limited formal systems of transportation, communication, and financial markets. There are high rates of food insecurity, poverty, and unemployment in the population; many people survive on subsistence farming and herding, income generated through work in the informal sector, and remits from labor migration to more urban areas (County Government of Kwale, 2018). A Kenyan NGO, The Nikumbuke Project, was established in Lunga Lunga as a development initiative to enhance women’s social capital and promote gender equality. Supported by the Swedish nonprofit, From One to Another, and the US-based Health by Motorbike, the Nikumbuke Project provides basic literacy training and health education for its adult female members and school-fee subsidies for their daughters. In addition to these core activities, the NGO offers a training program in tailoring for women who did not complete secondary school and workshops on family planning, gender-based violence, and sexual and reproductive health; the organization has encouraged the construction of town halls in each community as sites for regular meetings of its Nikumbuke members and other local activities, and has worked with communities to install water tanks in areas where access to water is limited. At the time of this study, the Nikumbuke Project was operational in 10 communities that represent a diversity of religions (Catholic, Muslim, traditional, and other) and tribal groups living in seven settled villages, a Maasai pastoralist community, a mixed pastoralist/settled village, and Lunga Lunga, a market town and the seat of the sub-county in which these communities are located. Tribal and ethnic identities are important in Kenya, and communities in this study are generally organized around these attributes. The communities are spread across the sub-county and several are located as far away as 40 kilometers from the Nikumbuke headquarters. Although several villages are situated along the paved roadway used for transporting goods between Kenya’s major port city, Mombasa, and Dar es Salaam in Tanzania to the south, most roads within and between villages are unimproved paths. Residents commonly travel between villages on foot or by motorbike, and paths can become impassable during the rainy seasons for all but foot traffic.
In 2012, an American varsity athlete who was part of a six-week university study abroad program affiliated with the Nikumbuke Project decided to play pick-up soccer with the local children as part of her exercise regimen. To everyone’s surprise, the women members of the Project, some of whom had either played soccer as students themselves or had children currently playing soccer in school, enthusiastically joined in. Later that year, the Nikumbuke Project membership requested that it be given the opportunity to start its own soccer league. Believing that such a league would contribute to its health and wellness goals, the Project leadership asked the same American student for assistance in setting up the new league. In 2014, she established a US-based nonprofit, the Nikumbuke Soccer League, to offer guidance and support for an all-women’s adult recreational soccer league, the first of its kind in Kenya. In 2019, at the time of the study, each of the ten villages in the Nikumbuke Project hosted a team of 22-23 players selected by the Nikumbuke members in that village.
Quantitative Phase
A semi-structured survey instrument was used to collect cross-sectional data in the quantitative phase of the study. It contained questions relating to demographics, health, gender norms, soccer participation, and access to social support. Before the survey launch, members of the research team attended a regular meeting of each village group to introduce the study and develop a contact list for follow-up recruitment. Prior to the start of data collection, project members in each community were asked to nominate individuals to serve as a member of the local data collection team. From these nominees, the study team assembled a team of women who were able to read and write and were fluent in Swahili; many of them had experience serving as “teachers” in the Project’s regular literacy programs. They participated in a week-long training program in research ethics and survey techniques run by the study team and practiced both consent procedures and survey administration using role-play exercises. Data collectors received a small stipend for successfully completing their training (500 Kenyan shillings [KES]—approximately $5 in U.S. dollars) and for each survey they administered (300 KES). The contact list created at the introductory meetings in each community was used by the study team to schedule individual visits with women who were interested in participating. Women who agreed to participate in the survey were also given a small compensation (200 KES). The surveys took between 35-65 minutes to complete and were administered by the local data collectors in a private setting, quiet corners of the village halls, or respondents’ homes. Surveys were checked by members of the study team at the end of each day to flag any methodological errors and to identify any data collectors who might be having difficulty with aspects of survey administration. Although available in both English and Kiswahili (the official languages of Kenya), the majority of surveys were administered in Kiswahili. Data collectors in the two communities that were home to Maasai were also able to translate questions verbally into Maa (the language of the Maasai people) as needed. Two members of the study team who live in Kenya and are fluent in Kiswahili and English, moved among the ten communities at the beginning of and throughout data collection and were available to answer questions, review completed surveys, and provide guidance where needed.
Sample
All 702 women who were members of the Nikumbuke Project, including members who played soccer in the league (229) as well as those who did not (473), were invited to participate in the quantitative portion of the study, and there were no refusals recorded. To be eligible, members had to be 18 years or older and able to provide verbal informed consent. The local data collectors, who had completed the surveys as part of their training, were excluded from the final sample of 684 women.
Measures
The outcome variable of interest was perceived social support from friends (PSF), measured by women’s responses to five questions about their perceived ability to access different kinds of support from friends when needed: emotional support, food, money, shelter, and someone with whom to talk about important matters. Responses to each item were recorded on a three-level Likert scale reflecting agree, partially agree, or disagree. Women were asked whether they participated in other groups besides the Nikumbuke Project, and to indicate their level of agreement with two additional questions: “most of my friends come from my village/community”, and “I have friends in other villages/communities”. Women were also asked to indicate, using a five-point scale ranging from none of the time to all of the time, the frequency in the past four weeks in which emotional or physical health had interfered with social activities. Sociodemographic measures were also included to record age, number of children, relationship status, education, village of residence, and household headship. Based on reported village of residence, a variable type of village was created to indicate whether the respondent resided in the pastoralist community, a settled village, the mixed pastoralist/settled community, or the market town.
Analysis Plan
Data analyses were conducted using StataCorp statistical software, Release 16 (StataCorp, 2019). An exploratory factor analysis (EFA) was conducted to determine if the five separate questions relating to whether a woman had friends on whom she could rely for various resources could be used as a single measure of perceived support from friends (PSF). For this purpose, listwise deletion was used to eliminate those respondents for whom responses to one or more of the five support questions were missing; this resulted in an EFA-analytic sample of 673 respondents. The sample was found to meet the threshold for factor analysis as recommended by Hair et al. (1998), with an average inter-item correlation of .37, Kaiser-Meyer Olkin Measure of Sampling Adequacy of 0.75, and significant Bartlett’s Test of Sphericity (χ2 (10, n=673) = 744.23, p < .001). Principle components analysis revealed only one factor with an eigenvalue greater than one, suggesting a simple structure with all five items loading strongly onto that factor. This factor explained 50% of the variance with factor loadings from .65 to .79. The five-item scale had a Cronbach’s alpha of 0.75. (see Table 1).
Table 1 – Items included in ‘perceived support from friends’ (PSF) scale*
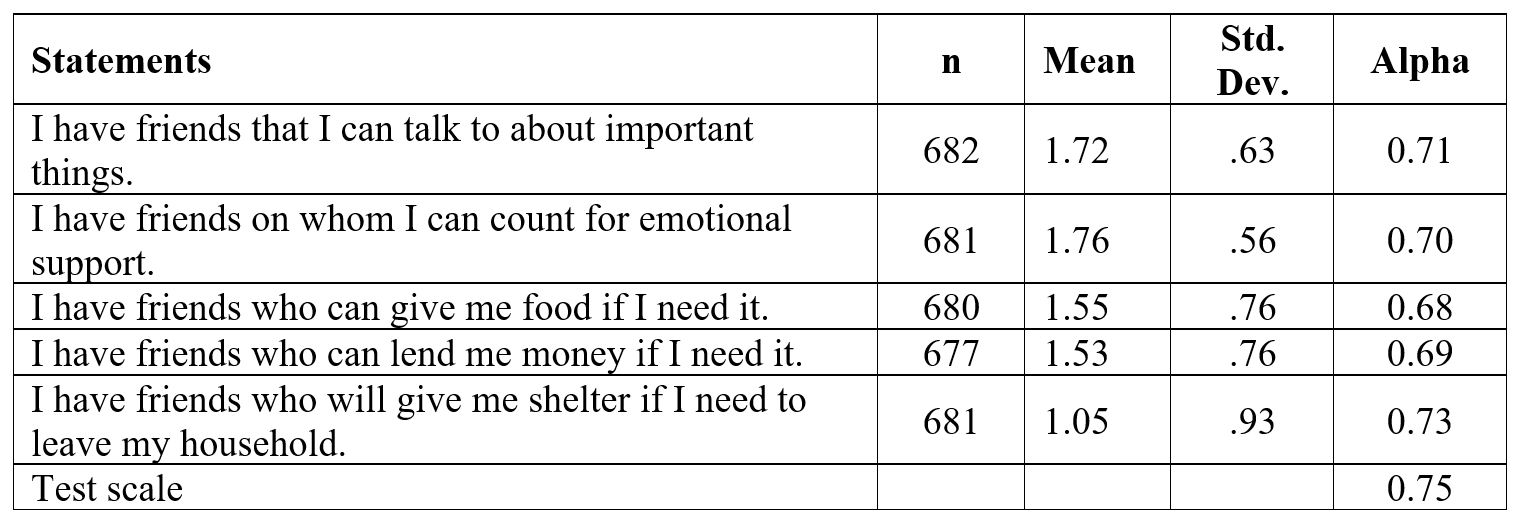
* Possible values of responses for individual items ranges from 0 to 2, with 2=Agree, 1=Partially agree, and 0 = Disagree
Each item had a value ranging from 0 to 2; the scale was scored as a summed total of the values for all five items. For bivariate and multivariate analyses, a binary variable perceived social support was created to reflect whether respondent scores on the PSF scale were lower than/equal to or higher than the mean score of the sample. Frequencies were computed for all study variables. Separate Pearson’s chi-square tests of independence were run to explore bivariate relationships between level of perceived social support, participation in the soccer league, and sociodemographic attributes.
Two multivariate regression models were used to examine the relationship between women’s PSF and their participation in soccer. The first was a linear model containing the continuous variable PSF, with values ranging from 1 to 15 as the dependent variable; the second used a dichotomous variable indicating social support that fell either above the mean/at or below the mean. An item non-response analysis of the sample surveys indicated minimal missing data on all variables less than 5% except for age (9.5%). Missingness among the five items comprising the PSF scale ranged from 0.29% to 1.2%. For the regression analyses, multiple imputation was used to approximate missing data for all variables included in the model. Values for age were not imputed given the large percentage of missing values (9.5%), nor was age, given its lack of statistical significance at the bivariate level with perceived social support, included in the multivariate models. Variance inflation factors (VIF) for all variables included in the models were less than 1.5, well below the generally accepted threshold indicating multicollinearity (Hair et al., 1998). The strength and direction of the relationships between the independent and the dependent variables were similar in both the linear and logistic regression models. As many of the independent variables were categorical, the logistic regression model was somewhat easier to interpret and those findings are reported here.
Qualitative Phase
The qualitative phase took place five months after collection and preliminary analysis of the quantitative data. Exploratory sequential mixed methods research utilizes findings from an initial quantitative phase to shape the design, sample, and questions that will comprise a follow-on qualitative phase (Creswell & Creswell, 2017). In this study, the quantitative data suggested a significant relationship between women’s participation in the soccer league and high social support (see Table 2). To explore this relationship further, the qualitative phase of the study involved a purposeful sample that included only women from the Nikumbuke Project who played in the soccer league.

All members of the soccer league (N = 229) were invited to participate in the focus group discussions (FGDs), which were facilitated in Kiswahili by the third and fourth authors. At the start of each FGD, the facilitators explained the purpose of the FGD, how the session would be organized, and asked for women’s oral consent to participate and be video recorded for the purpose of transcription. Each participant received a modest compensation of 100 KES for their time. Although the FGDs were to be facilitated primarily by the study team, it was decided that Nikumbuke members who had served as data collectors during the quantitative phase of the study would benefit from the opportunity to receive training, assist in the coordination of the discussions and, where needed, translate into the Maasai language. Training sessions were held to review study goals and objectives, ethical issues relating to focus groups, and qualitative data collection. Trainees received a stipend of 300 KES for successful completion of the qualitative training program and for their participation in focus-group facilitation.
Two focus-group discussions of 10-13 players each took place in each of the ten Nikumbuke communities to allow all members in that community’s soccer team the opportunity to participate without the FDGs becoming unwieldy. Each FGD lasted approximately 90 minutes. Sessions followed a script containing open-ended questions about women’s motivations in joining the soccer league and the ways in which playing on the team had affected their general health, their relationships, and their roles in the community. Eighteen of the sessions were conducted in Kiswahili and two in the Maasai language.
Video recordings of sessions conducted in Kiswahili were first transcribed into Kiswahili and subsequently translated into English by a transcription service in Nairobi. Video recordings of the two sessions conducted in Maa were simultaneously transcribed and translated directly into English by a language instructor in Nairobi fluent in Maa, Kiswahili, and English. An error in videotaping during two of the focus groups necessitated the omission of these sessions from the analysis. The resultant analytic sample included data from two FGDs comprising members from each of eight teams and one FGD from each of the two teams in which the videotaping errors had occurred, for a total of 201 women. All qualitative analyses were performed in NVivo 12 using the English translations (QSR International, 2018).
Analysis Plan
The qualitative phase used a thematic analysis approach to identify and interpret patterns in the data (Braun & Clarke, 2006). The study team members responsible for analyzing the qualitative data included the first author (the project’s primary investigator, who has over seven years’ experience in working with the Nikumbuke Soccer League), and the second author, a team member familiar with the setting and an experienced qualitative researcher. These authors, neither of whom speak Kiswahili, consulted with team members who were fluent in Kiswahili in those instances where interpretation of the underlying meaning of a translated phrase was not clear. First, they familiarized themselves with the data by reviewing each transcript, drafted a list of initial codes independently, and then met to generate a common set of codes. Next, each reader coded two focus groups independently and then compared coding choices to review and refine the codebook. Using this revised codebook, each reader independently coded six of the focus groups to assess interrater reliability. Interrater reliability (Cohen’s kappa) was, on average, 97% and ranged from 94-99%. The two readers met to align code definitions. Both then independently finished coding the remaining focus groups, discussing issues as they did so. Focusing on the theme of social support, the two met frequently to further refine, name, and define the theme and sub-themes, and to ensure interrater reliability. Qualitative findings were then presented to the remaining five authors, including those authors who had facilitated the focus groups (third and fourth authors). All authors collaborated on the interpretation of the findings.
RESULTS
Quantitative Findings
Descriptive statistics and findings from the bivariate analyses are reported in Table 3. The majority of respondents were between the ages of 25 and 49 years, married with 3 to 5 children, and lived in settled villages. Nearly 40% of respondents had no formal education and another 30% had not completed primary school. Slightly more than one-third of respondents played in the soccer league. Two-thirds or more of the respondents agreed that they had friends on whom they could count for money, emotional support, food, and conversation about important things when needed. Fewer than half of respondents perceived that they had friends who could give them shelter if needed. Summed scores on the PSF scale ranged in value from 0 to 10, with more than one third of respondents perceiving that they would have support from friends on all five items if needed. The mean and median scores for the scale were 7.56 (standard deviation 2.61) and 8.0, respectively; mean scores and response percentages for each item in the scale are reported in Table 1. Nearly two-thirds of respondents had aggregate scores for the PSF scale that were above the mean score. In the bivariate analyses all variables except “type of village” and “participation in other groups” were significantly associated with participation in the soccer league (Table 3). Type of community, participation in soccer, having friends from one’s village, and having friends from outside one’s village were significantly associated with perceived social support.
Soccer team participation, type of village, having friends from one’s village, and having friends from outside one’s community significantly increased the odds of having perceived social support scores above the sample mean after controlling for covariates. Women who played in the soccer league had nearly double the odds of reporting high perceived social support compared to their non-soccer peers (OR 1.98, CI95 1.37, 2.86, p < .001).

Qualitative Findings
Four central themes emerged during the focus group discussions concerning women’s participation in the soccer league and their perceptions of its benefits: friendships within and between communities, teambuilding and collaboration, emotional and instrumental support on and off the field, and reduced stress and anxiety. Quotes from focus group participants are utilized throughout this section as thematic headings and to underscore the findings’ trustworthiness (Creswell, 2013).
“We make a lot of friends when we go to play soccer.” (JIW1-R12)
A number of women expressed that they had few friends prior to joining the soccer league and were lonely. They reported that soccer provided an opportunity to meet and make friends that was otherwise not available to them.
Before I joined the team, I only had one friend- she could not help me much. But after I joined, I made many new friends. I can no longer talk about going back to my mum and dad, I now have friends to whom I can go who are my team. (GOW1-R10)
I only had my neighbor as a friend; now I have the whole team as my friends, even some I do not know where they live, but they are my friends. (MPW1-R7)
References to not knowing another woman’s “home” before playing soccer were common. Women reported that soccer had enabled them to meet and form friendships with women from outside their own communities.
It helps with friendships because you can meet someone in the group and yet you do not even know their home. You meet here and build friendships until you get to know their home and they yours. Maybe they come from Kibaoni and you are from Mgombezi, but when you meet, you become friends. (MGW2-R4)
We used to have friends only from this locality, and now we have made friends from far places like Lunga Lunga. Therefore this has brought unity. Therefore we have seen that we have peace. (MAW1-R9)
“You fall down, hold your friend’s hand, and stand.” (KIW1-11)
As a team sport, soccer requires coordination, communication, and trust among team members. Acknowledging the importance of teamwork, women discussed high levels of encouragement and support among players. Women celebrated each other’s improvements and successes, creating an environment that was often described as joyful and festive. As one woman put it, “As we play, that teamwork and coordination brings us to one level and it feels so good and makes us laugh a lot” (MW1-R11). Women observed that even when they had arguments with team members off the field, or things went badly on the field, they maintained their bonds and set arguments aside so that they could move forward together as a team. Women described helping each other up after a fall and helping each other improve. Women described forming friends with other players on their team and opposing teams because they would ask other women for help with soccer skills. As one woman explained:
When you go to play soccer and see a good player, you will want to stay close to her to know how she started. Perhaps she will tell you that she started by going to see another team play. She can also give you advice that will enable you to help someone else. (JIW1-R2)
In addition to friendships arising from a woman’s admiration for another woman’s soccer skills, face-to-face competition in soccer created bonds between women: “You know that this is the one that we were fighting for the ball together with. Yes, you get to know each other” (PEW1-R11). As opposed to being adversarial, going head-to-head with an opposing player increased social support and connection for women in the soccer league. “And us, when we play, even if it is hitting my friend, when we have ended the game, I will sit close to her. I tenderly care for that leg and show that friendship so that she knows it wasn’t on purpose” (PEW2-R5).
Across focus groups, women frequently echoed some form of the sentiment “When we get to the fields there are no tribes” (MGW2-R12). Women described how one could not focus on who was in one’s tribe while playing soccer because one had to focus on who was on one’s team and open to receive the ball. Women saw tribalism as disrupting the success of their teams: “If we were tribal as a team, we would not be confident, but since we are [confident], we trust each one of us is going to play their best” (KIW1-R1). As one respondent put it, “we cannot focus on the Digo or Duruma (two different tribal groups in the area); here, we are all equal” (LUW1-Respondent 8). Teamwork and its by-products of trust and interdependency created family-like bonds among the women, who frequently shared the idea that “we have become just like sisters” (PEW1-R1).
Women shared that sister relationships built between women during soccer transcended their village- and tribal-identities and “brought harmony between us and our neighbors” (MAW1-R2). As one participant put it, “When we are in the pitch we are all sisters and nobody cares about tribe. … you will often find two people from different areas becoming close friends” (GOW2-R11). A number of women spoke about the benefits of competing against teams from other communities and how doing so helped them to learn new things.
And something else, the sport for me has brought me together with many people from different areas…. We meet with them, we get to talk and know about other things from those living elsewhere and what they do there. I mean it has helped us to meet up associating with each other and getting to know different things. Now for me there are places that I did not know but I have now known due to going for the sport. (LUW1-R13)
“We lean on each other as a group for support.” (MPW1-R1)
Throughout the focus groups, women discussed the emotional support they received from other players. Women described how soccer created the opportunity for them to share their problems with other women and get “lifesaving advice” (JUW1-R1) from one another. As one woman described it: “I have friends, therefore I made networks, in going out and seeing newer things and meeting mothers with diverse thoughts. We sat down and shared; it really changed my life” (PEW2-R8). When women met and an issue arose, “we handle[d] it together” (LUW2-R9). The friendships women described were marked with listening, empathy, and reciprocity: “Yes, it has strengthened the bond. We have become like siblings. When one of us has a problem, we come together and sort it out. We have grown to have strong ties” (MPW2-R9). Importantly, women also pointed to connecting with women from other villages as having helped them gain new insights. Some women shared that being part of the soccer community had connected them to women who “willingly advise us on how we can grow ourselves economically” (MPW1-R1).
[My teammates] also help in suggesting to me ways of attracting income. For example, when I come here, one may tell you, “when coming here to this group of people for sports, you can even come with your half cakes and visheti [sweet pastries]. You make something for the bus”. So if I make that and come with them here when I go back, I have made some money. I can buy some salt. I can do something. If it were not for ball, where would I have gotten that? (LLW1-R5).
In addition to emotional support and advice, women discussed the instrumental support that they received from fellow soccer players.
And you help each other a lot because, even if you have a problem, when you meet with your fellow women, you can explain it to them, and you all talk about it as friends and sisters. When you say “I am really troubled, I need your help”, your friends will come together and help you. Even if it is watching over your child, your friends can help you. (GOW1-R10)
It has been good for us who play football. We can meet here and I let my team members know that I need financial assistance of about 10,000 KES [approximately $90 U.S. dollars]. The friendship in the group has really helped. When I ask for something, even if not everyone will chip in, you cannot fail to get one or two people who are willing to help. (MGW2-R6)
“When you mix with your friends, all the stress is gone.” (LUW2-R6)
Women described being largely alone prior to joining the soccer league, left to figure out their problems by themselves. Through the friendships forged through soccer, the women have gained an outlet for their worries and problems, which they report has in turn reduced stress and anxiety. Women remarked that the fun and camaraderie associated with playing soccer dispel women’s worries.
If you go to the field when you are stressed, maybe someone made you angry, you are thinking, but when you get to the others, the talking and laughing, when you are out of the field, you are stress free, your mind is busy with better thoughts. (JUW1-R5)
As another participant described her experiences:
I used to have very many thoughts when I was alone at home, but once I come and sit with my friends here, then I feel relaxed and go home satisfied. This group has brought us together and is very helpful, not only in matters of football, but also in life problems. I get to share with my friends the issues affecting me and they help me out. It is not that we have no stress or worries, but we just struggle and make it. (PEW1-R3)
Across focus groups women discussed how the social support they had from their teammates decreased their worries and stress, and made them realize that they were not alone in their problems. “We women do not hide anything from each other, so in the conversations on the field we are able to free up. When I am annoyed and get on the field, the anger goes away immediately and I change completely” (PEW2-R4).
Many of the women talked about stress at home and the problems they face as wives and mothers. Although the problems were still there when they returned home from soccer, women found that they worry less about them and recognize that soccer provides an outlet for their anxiety: “When one plays football, one is able to handle the challenges that come from raising children and marriage” (KIW1-R11). As one woman commented:
Some of us could not leave the house to go meet other women, or some were always stressed, do you understand? But right now she is able to leave home and cooperate with others. She has the opportunity to talk to other women, and that has changed her thoughts. Maybe she was angry because of the excess duties or children every time, but right now she leaves the house, her thoughts are lost out there [on the soccer field] and she comes back home with a fresh mind. (JUW2-R2)
DISCUSSION
This study used a mixed methods approach to examine the nature of and extent to which the women’s soccer league contributes to the development goals of enhancing social support, building community cohesion, and improving women’s emotional and physical health in rural Kenya. Although the physical and psychosocial benefits of team sports are well-documented in the literature and sports programs have been used with considerable success elsewhere in Kenya to build the social assets of adolescent girls (Brady, 2005; Brady & Khan, 2002; Forde, 2009), very little was known prior to the current study about the benefits of recreational team sports for adult women in Sub-Saharan Africa. Findings confirmed the first two hypotheses in this study: that adult women who play soccer in this setting have higher social support than their non-soccer playing peers, and that the nature of team sport, itself, contributed to building strong perceived social support from friends. Although most women in the Nikumbuke Project reported in the quantitative phase that they had friends, the PSF-scale data would suggest that project members who played in the soccer league had greater odds of feeling that they had friends on whom they could depend for emotional and instrumental support when needed. Because playing soccer required teamwork and interaction with women on other teams, the league created both an enabling environment in which women met and formed friendships and a social space in which they built a network of peers with whom to share their worries. It provided an opportunity for women to share ideas, learn from each other about income-generating activities, and ask for help with childcare, transportation, and expenses when needed. This social network included not only one’s team members but extended across teams, villages, tribal affiliations, and religions. This finding is consistent with prior work elsewhere that found team sports to be effective mechanisms for building social capital in women (Ottesen et al., 2010). Friendship, competition, and fun experienced as part of belonging to the league in turn reduced stress and anxiety (see Table 2).
Quantitative results suggested that having friends within and outside one’s community, membership in a pastoralist community, and playing soccer were positively associated with perceived social support from friends, controlling for other attributes. It is not surprising that having friends is a significant predictor of women’s perceived social support from friends, given that one would not have social support from this source if one did not first have friends on which one could or could not rely. The majority of women who participated in the surveys reported having friends, both near and far, irrespective of their participation in the soccer league. There are a number of possible explanations for these findings. All survey respondents were members of the Nikumbuke Project. The project provides a social space in which women, whether or not they play soccer, regularly come together in their communities for literacy training, health promotion meetings, and information sharing. Many of the women regularly attend churches, mosques, or other religious gatherings in their communities. Market days in Lunga Lunga draw women weekly from the surrounding communities to sell goods and/or purchase supplies, providing yet more opportunities for women to meet and to socialize.
Women from settled villages and the mixed settled/pastoralist community had significantly lower odds of PSF scores above the sample mean compared to women from the Maasai pastoralist community. This finding may be a reflection of differences in the spatial and non-spatial organization of these communities. Although contemporary Maasai communities in coastal Kenya and northern Tanzania are varied in the degree to which they have been affected by outside cultural and political forces, the Maasai community included in this study general adheres to traditional Maasai domestic and living arrangements. Most families live in boma, residential units that can comprise several independent households of related family members. Although each married man and his household may independently own cattle, grazing rights, control of land, and access to water are owned communally. The unity of a clan, a group sharing a common patrilineal ancestor, is symbolized using common cattle brands, and although more common at the level of the immediate family, clan members have mutual aid obligations to each other in times of need. Women are the de facto heads of houses and act with considerable autonomy with respect to domestic affairs, children and the family economy. This social organization, described as one of mutual dependence and obligations between men and women (Kipuri, 1989) is likely to reflect an environment in which women, in the sharing of daily responsibilities, feel that they can depend on each other. In the other, more settled communities included in this study, the tasks of household production and domestic duties often fall to an individual woman and her children and tasks are not shared in common among neighbors. Women bear responsibility for providing food for their families in an environment of scarcity, leaving them little time in which to socialize with other women. Although the Nikumbuke Project, religious gatherings, and market days create social opportunities for women in settled communities to mingle and form friendships with others, such friendships may not be characterized by the co-dependencies and sense of mutual obligation that were integral to the Maasai social structure observed in this study.
This distinction between acquaintances and friends on whom one can depend, may help to explain the observed differences in the quantitative findings between Nikumbuke Project members who played soccer and their non-soccer playing peers. These findings showed that being a member of the soccer league was significantly associated with scores above the sample mean on the PSF scale both in the bivariate analysis and in the multivariate model that controlled for other attributes. They validate the study’s first hypothesis that women who played soccer have greater perceived social support than their non-soccer playing peers.
Qualitative results provided granular data that helped explain the relationship between soccer and social support and confirmed the study’s second hypothesis. Soccer brought women together in an atmosphere of play and friendly competition; it created a time and space in which women could socialize and form friendships near and far. The friendships formed with peers on a soccer team were based on a shared experience and a collective identity. To play league soccer, women had to rely on each other to defend their team’s goal, to pass the ball to each other when there was an opening in play, and to shoot to score. Doing this well required that women set aside any differences they may have off the field and come together as a collaborative, supportive network. This shared social identity endured beyond the soccer pitch.
Women who participated in this study daily confront the challenges of poverty, the constant demand of household production and childrearing, and the gender norms that define their roles in their intimate relations, their households, and their communities. In this setting, it is quite possible that soccer is one of the few activities in which women can step away from their responsibilities and duties as wives and mothers. Women told the authors that soccer provided a social space for talking with other women, that games were fun, and that the atmosphere was often festive. Study findings suggest that women’s problems were set aside, but not resolved, during soccer. Nonetheless, playing soccer seems to offer a buffer between problems and the worries to which they give rise. This finding is in keeping with the buffering hypothesis put forward by Cohen and Wills (1985) which posits that social support acts as a buffer between stressful events and health outcomes, in this case stress and anxiety. Women commented that while problems persisted, they worried about them less when they returned home after playing soccer with their friends.
Friendships made and cemented through soccer gave women confidence that they had friends on whom they could rely for both emotional and instrumental support when it was needed; in turn, women felt less stress, even when confronting the same problems at home when they stepped back off the pitch. This finding also aligns with research on social support that found that these buffering effects were greater when women shared a social identity (Frisch et al., 2014; McKimmie et al., 2020). In this case, soccer provided a social identity for its team members as well as a shared activity whose structure encouraged mutual dependence and support among women. Focus group participants credited their being part of a soccer team and the support of friends made on the field with reduced feelings of stress and anxiety. Findings from this study offer foundational support for this study’s third hypothesis, suggesting that soccer leagues for adult women may be an effective intervention for building social support and improving women’s mental health. This may be especially true in settings in which other opportunities for women to step outside the demands of daily life are limited.
Study Limitations
It is important to note limitations in this study and directions for future research. The soccer league under study is embedded within a pre-existing development program that is widely endorsed by the participating communities. Community leaders, husbands, and family members accept that women spend some portion of time each week on Nikumbuke activities that yield benefits to households and communities. Under such circumstances, the setting aside of chores and responsibilities by women to engage in sport may not be viewed as idleness or time wasted in play but rather as part of a larger community-level enterprise. The Nikumbuke Project as a whole is widely viewed as a positive force in the communities and by the women it serves. Many project members, particularly those women who work directly with the program in the provision of literacy training and health information, welcomed the research as an opportunity to support the project and to share their experiences. Members’ positive attitudes towards the Nikumbuke Project are likely to have contributed to the high participation rate in the study and may have encouraged women to respond to study questions in ways they felt would reflect favorably on the program. In addition, the soccer league was established at the explicit request of women in the Nikumbuke Project; whether a free-standing women’s soccer league that is not demand-driven or part of a broader program of activities would enjoy the same success in building social support for women is not known. Despite strong evidence that emerged in the focus group discussions about the positive role that soccer plays in overcoming loneliness, building social support, and reducing stress, causal or temporal inferences about the effects of the league on individual levels of PSF could not be derived from the cross-sectional survey data. Longitudinal studies of soccer leagues begun de novo elsewhere or of new teams forming in the future under the Nikumbuke Project would allow for further testing of the PSF scale, and be useful in building an evidence base on the effects of soccer participation on women’s social support and its role as a social development tool.
CONCLUSION
Social support has been widely recognized for its positive effects on health and well-being. Recreational team sports, while often adopted as strategies to build social support and enhance well-being among adolescent girls and young women, have to date been underutilized as a sport-for-development intervention to improve the emotional health and well-being of adult women, particularly in lower- and middle-income countries. Evidence from this study suggests that adult women’s participation in recreational soccer is positively associated with perceived social support from friends, and that participation in team sports directly contributes to building friendships and social support which, in turn, reduce stress and anxiety in women’s daily lives. Given the popularity of soccer in many parts of the Global South and the low costs associated with initiating such programs in rural areas, gender-development programs should consider introducing recreational soccer activities for adult women in under-resourced settings where more complex and costly initiatives may be difficult to implement or sustain.
FUNDING
This study is part of a large mixed-methods study supported by grants from Patrick Byrne, Adidas North America, and the United States Department of State, Kenya. The study received in-kind support from Rutgers University-Division of Intercollegiate Athletics, the Nikumbuke Soccer League-US, the Sports Bra Project, and the Nikumbuke Project-Kenya.
ACKNOWLEDGEMENTS
Special thanks are due the Nikumbuke Soccer League-US, Ken Wakia at the US Embassy in Kenya, and the many individuals at Rutgers University who contributed in various ways to making this research possible. Of particular note are Frances Loeser, Keri Ferreira, Patrick Hobbs, Dennis DeMarino, Asenath Dande, and the Rutgers Global staff. This study would not have been possible without the enthusiastic participation of the staff of the Nikumbuke Project in Lunga Lunga, and the remarkable women of Nikumbuke. A special note of gratitude is due the Nikumbuke teachers who assisted with data collection and focus group coordination.
REFERENCES
Akindes, G., & Kirwin, M. (2009). Sport as international aid: Assisting development or promoting under-development in Sub-Saharan Africa? In R. Levermore & A. Beacom (Eds.), Sport and International Development. Global Culture and Sport. (pp. 219-245). Palgrave MacMillan. https://doi.org/10.1057/9780230584402_10
Barchi, F., AbiNader, M. A., Winter, S. C., Obara, L. M., Mbogo, D., Thomas, B. M., & Ammerman, B. (2021). “It is like medicine”: Using sports to promote adult women’s health in rural Kenya. International Journal of Environmental Research and Public Health, 18(5), 2347. https://doi.org/10.3390/ijerph18052347
Barchi, F., Winter, S.C., Mbogo, D., Thomas, B., & Ammerman, B. (2022). Exploring the relationship between participation in an adult-women’s soccer league and intimate partner violence in rural Kenya. Journal of Interpersonal Violence, 37(9-10), NP7907-NP97931. http://doi.org/10.1177/0886260520969241
Berkman, L. F., & Glass, T. (2000). Social integration, social networks, social support, and health. In L. F. Berkman & I. Kawachi (Eds.), Social Epidemiology (pp. 137-173). Oxford University Press.
Bloom, J. R. (1990). The relationship of social support and health. Social Science & Medicine, 30(5), 635-637. https://doi.org/10.1016/0277-9536(90)90162-L
Brady, M. (2005). Creating safe spaces and building social assets for young women in the developing world: A new role for sports. Women’s Studies Quarterly, 33(1/2), 35-49.
Brady, M., & Khan, A. B. (2002). Letting girls play: The Mathare Youth Sports Association’s football program for girls. Population Council
Braun, V., & Clarke, V. (2006). Using thematic analysis in psychology. Qualitative Research in Psychology, 3(2), 77-101. https://doi.org/10.1191/1478088706qp063oa
Breet, E., Kagee, A., & Seedat, S. (2014). HIV-related stigma and symptoms of post-traumatic stress disorder and depression in HIV-infected individuals: Does social support play a mediating or moderating role? AIDS Care, 26(8), 947-951. http://doi.org/10.1080/09540121.2014.901486
Chandran, A., Benning, L., Musci, R. J., Wilson, T. E., Milam, J., Adedimeji, A., Parish, C., Adinora, A. A., Cocohoba, J., Cohen, M. H., Holstad, M., Kassaya, S., Kempf, M-C, & Golub, E. T. (2019). The longitudinal association between social support on HIV medication adherence and healthcare utilization in the Women’s Interagency HIV Study. AIDS and Behavior, 23, 2014-2024. https://doi.org/10.1007/s10461-018-2308-x
Cobb, S. (1976). Social support as a moderator of life stress. Psychosomatic Medicine, 38(5), 300-314. https://doi.org/10.1097/00006842-197609000-00003
Cohen, S., & Syme, S. L. (1985). Social support and health. Academic Press.
Cohen, S., & Wills, T. A. (1985). Stress, social support, and the buffering hypothesis. Psychological Bulletin, 98(2), 310-357. https://doi.org/10.1037/0033-2909.98.2.310
County Government of Kwale. (2018). Kwale County Integrated Development Plan (2018-2022). Kwale County, Kenya: County Government of Kwale. https://repository.kippra.or.ke/bitstream/handle/123456789/417/2018-2022-Kwale%20County%20CIDP.pdf?sequence=1&isAllowed=y
Creswell, J. W. (2013). Qualitative inquiry: Qualitative inquiry and research design. SAGE.
Creswell, J. W., & Creswell, J. D. (2017). Research design: Qualitative, quantitative, and mixed methods approaches. SAGE.
del-Pino-Casdo, R., Frias-Osuna, A., Palomino-Moral, P. A., Ruzafa-Martinez, M., ramos-Morcillo, A. J. (2018). Social support and subjective burden in caregivers of adults and older adults: A meta-analysis. PloS One, 13(1), Article e0189874. https://doi.org/10.1371/journal.pone.0189874
Forde, S. (2009). Playing by their rules: Coastal teenage girls in Kenya on life, love, and football. CreateSpace.
Frisch, J. U., Häusser, J. A., van Dick, R., & Mojzisch, A. (2014). Making support work: The interplay between social support and social identity. Journal of Experimental Social Psychology, 55, 154-161. https://doi.org/10.1016/j.jesp.2014.06.009
Gyasi, R. M., Phillips, D. R., & Abbas, K. (2019). Social support and psychological well-being in community-dwelling older Ghanian cohorts. International Psychogeriatrics, 31(7), 1047-1057. http://doi.org/10.1017/S1041610218001539
Hair, J. F., Anderson, R. E., Tatham, R. L., & Black, W. C. (1998). Multivariate data analysis (5th ed.). Prentice Hall.
Hancock, M., Lyras, A., & Ha, J.-P. (2013). Sport for development programs for girls and women: A global assessment. Journal of Sport for Development, 1(1), 15-24.
Harandi, T.F., Taghninasab, M. M., & Nayeri, T. D. (2017). The correlation of social support and mental health: A meta-analysis. Electronic Physician, 9(9), 5212-5222. http://doi.org/10.19082/5212
Huggins, A., & Randell, S. (2007, April). The contribution of sports to gender equality and women’s empowerment [Conference presentation]. International Conference on Gender Equity on Sports for Social Change, Kigali, Ruwanda. https://citeseerx.ist.psu.edu/viewdoc/download?doi=10.1.1.517.2234&rep=rep1&type=pdf
Ivankova, N. V., Creswell, J. W., & Stick, S. L. (2006). Using mixed methods sequential explanatory design: From theory to practice. Field Methods, 18(1), 3-20. http://doi.org/10.1177/1525822X05282260
Jeanes, R. (2013). Educating through sport? Examining HIV/AIDS education and sport-for-development through the perspectives of Zambian young people. Sport, Education and Society, 18(3), 388-406. https://doi.org/10.1080/13573322.2011.579093
Johnson, R. B., Onwuegbuzie, A. J., & Turner, L. A. (2007). Toward a definition of mixed methods research. Journal of Mixed Methods Research, 1(2), 112-133. http://doi.org/10.1177/1558689806298224
Kalomo, E. N. (2018). Associations between HIV-related stigma, self esteem, social support, and depressive symptoms in Namibia. Aging & Mental Health, 22(12), 1570-1576. http://doi.org/10.1080/13607863.2017.1387763
Kipuri, N. (1989). The Maasai in transition: Class and gender in the transformation of a pastoral society. [Unplublished doctoral dissertation]. Temple University.
Lakey, B., & Cohen, S. (2000). Social support theory and measurement. In S. Cohen, L. G. Underwood, & B. Gottlieb (Eds.), Social support measurement and intervention: A guide for health and social scientists (pp. 29-52). Oxford University Press. https://doi.org/10.1093/med:psych/9780195126709.003.0002
Lazarus, R. S. (1966). Psychological stress and the coping process. McGraw-Hill.
Lyras, A., & Hums, M. A. (2009). Sport and social change: The case for gender equality. Journal of Physical Education, Recreation & Dance, 80(1), 7-21.
Lyras, A., & Welty Peachey, J. (2011). Integrating sport-for-development theory and praxis. Sport Management Review, 14(4), 311-326. https://doi.org/10.1016/j.smr.2011.05.006
Machisa, M., Christofides, N., & Jewkes, R. (2018). Social support factors associated with psychologixal resilience among women survivors of intimate partner violence in Gauteng, South Africa. Global Health Action, 11(sup3), Article 1491114. https://doi.org/10.1080/16549716.2018.1491114
McDowell, T. L. & Serovich, J.M. (2007). The effect of perceived and actual social support on the mental health of HIV-positive persons. AIDS Care, 19(10), 1223-1229. http://doi.org/10.1080/09540120701402830
McKimmie, B. M., Butler, T., Chan, E., Rogers, A., & Jimmieson, N. L. (2020). Reducing stress: Social support and group identification. Group Processes & Intergroup Relations, 23(2), 241-261. http://doi.org/10.1177/1368430218818733
Meier, M. (2000). Gender Equity, Sport and Development. Swiss Academy for Development.
Na, M., Miller, M., Ballard, T., Mitchell, D.C., Hung, Y.W., & Melgar-Quiñonez, H. (2018). Does social support modify the relationship between food insecurity and poor mental health? Evidence from thirty-nine sub-Saharan African countries. Public Health Nutrition, 22(5), 874-881. http://doi.org/10.1017/S136898001800277X
Noret, N., Hunter, S. C., Rasmussen, S. (2020) The role of perceived social support in the relationship between being bullied and mental health difficulties in adolescents. School Mental Health, 12, 156-168. http://doi.org/10.1007/s12310-019-09339-9
Ong, H. L., Vaingankar, J. A., Abdin, E., Sambasivan, R., Fauziana, R., Tan, M-E., Chong, S.A., Goveas, R.R., Chiam, P. C., & Subramaniam, M. (2018). Resilience and burden in caregivers of older adults: Moderating and mediating effects of perceived social support. BMC Psychiatry, 18, Article 27. http://doi.org/10.1186/s12888-018-1616-z
Osborn, T. L., Venturo-Conerly, K. E., Wasil, A. R., Schleider, J. L., & Weisz, J. R. (2020). Depression and anxiety symptoms, social support, and demographic factors among Kenyan high school students. Journal of Child and Family Studies, 29, 1432-1443. https://doi.org/10.1007/s10826-019-01646-8
Ottesen, L., Jeppesen, R. S., & Krustrup, B. R. (2010). The development of social capital through football and running: Studying an intervention program for inactive women. Scandinavian Journal of Medicine & Science in Sports, 20(1), 118-131. https://doi.org/10.1111/j.1600-0838.2010.01123.x
QSR International. (2018). NVivo Qualitative Data Analysis Software (v.12). QSR International.
Richards, J., & Foster, C. (2013). Sport-for-development interventions: Whom do they reach and what is their potential for impact on physical and mental health in low-income countries? Journal of Physical Activity and Health, 10(7), 929-931. https://doi.org/10.1123/jpah.10.7.929
StataCorp. (2019). Stata Statistical Software: Release 16. StataCorp, LLC.
Taylor, S. E. (2011). Social support: A review. In H. S. Friedman (Ed.), The Oxford Handbook of Health Psychology (pp. 189-214). Oxford University Press. https://doi.org/10.1093/oxfordhb/9780195342819.013.0009
Tsai, A. C., Tomlinson, M., Comulada, W. S., & Rotheram-Borus, M. J. (2016). Food insufficiency, depression, and the modifying role of social support: Evidence from a population-based, prospective cohort of pregnant women in peri-urban South Africa. Social Science & Medicine, 151, 69-77. https://doi.org/10.1016/j.socscimed.2015.12.042
Uchino, B. N. (2006). Social support and health: A review of physiological processes potentially underlying links to disease outcomes. Journal of Behavioral Medicine, 29(4), 377-387. https://doi.org/10.1007/s10865-006-9056-5
Uweza Foundation. (n.d.). Uweza Soccer Academy. Uweza Foundation. Retrieved April 1 from https://uwezakenya.org/our-work/soccer-academy/
Wang, J., Mann, F., Lloyd-Evans, B., Ma, R., & Johnson, S. (2018). Associations between loneliness and perceived social support and outcomes of mental health problems: A systematic review. BMC Psychiatry, 18, Article 156. https://doi.org/10.1186/s12888-018-1736-5
Weber, S., Puskar, K. R., & Ren, D. (2010) Relationships between depressive symptoms and perceived social support, self-esteem& optimism in a sample of rural adolescents. Issues in Mental Health Nursing, 31(9), 584-588. http://doi.org/10.3109/01612841003775061
World Health Organization. (2003). Health and development through physical activity and sport. World Health Organization. https://apps.who.int/iris/handle/10665/67796
