Stacy Warner1, Emily Sparvero2, Stephen Shapiro3, Arden Anderson4
1 East Carolina University, Department of Kinesiology, USA
2 University of Texas, Department of Kinesiology and Health Education, USA
3 Old Dominion University, Department of Human Movement Sciences, USA
4 Texas A&M, Department of Health and Kinesiology, USA
Citation: Warner, S., Sparvero, E., Shapiro, S., Anderson, A. Yielding healthy community with sport? Journal of Sport for Development. 2017; 5(8): 41-52.
ABSTRACT
Research has linked an enhanced sense of community to sport programme retention, while literature outside of sport suggest increased sense of community is linked to improved health. Consequently, the purpose of this study was to better understand the association between sport communities and health behaviours and health role modelling outcomes. Athletes and non-athletes were surveyed to better understand the unique contributions sport participation might have on health-related outcomes. Surveys included demographic information, the 21-item Sense of Community in Sport scale, and various health behaviours and outcomes. Surveys were completed by 458 athletes and 323 university social organisation members (i.e., fraternities and sororities) in the United States. The results provided limited support for the positive influence of sense of community on health-related outcomes and indicated that athletes reported higher levels of sense of community (M = 75.17, SD = 10.158) than university social organisations participants (M = 72.17, SD = 12.134). When controlling for sense of community, surveyed athletes were more likely to engage in healthier behaviours (i.e., binge drink less, consider themselves role models in terms of exercise, maintain a balanced diet, and use less tobacco). This work highlights the community characteristics found in sport settings that can contribute to positive health outcomes.
INTRODUCTION
The association between sport participation and positive health outcomes is a complicated one that has been examined by researchers representing a variety of academic disciplines (e.g., sport management, public health). According to the World Health Organization, health is a multi-faceted concept that encompasses physical, mental, and social well-being.1 While sport participation has the potential to contribute to overall health,2-5 in some instances research suggests that sport demotes such salubrious outcomes.6-8 Despite this empirically supported criticism, sport participation is still commonly considered as a means to improve health. Any health improvement likely occurs because it is well-acknowledged that physical activity,which can be achieved through sport participation, is related to positive health outcomes.9.10 More specifically, at least 150 min of moderately intense physical activity per week is recommend for adults to achieve a health benefit.10 As trends demonstrate, less physical activity is being achieved daily through occupational (e.g., manual labour), domestic (e.g., household tasks), and transport (e.g., bicycling) means; interestingly, leisure-time physical activity (e.g., sports) has not declined.2,11
This suggests the existence of an opportunity for sport to be used for health-related benefits. Berg and colleagues2(p29) stressed the importance of participation in sport and physical activity, but noted that “sport is also not a panacea”, and exaggerating the power of sport can actually limit its use for public health policy. This is especially important because sport increasingly has been seen as an effective mechanism for community interventions designed to improve poor health.12 The exponential growth of sport for development initiatives worldwide and typically in disadvantaged settings and developing countries provides further evidence of this.13 Sport provides a potential means for delivering positive health outcomes, but how and under what conditions this occurs has not been made clear in the literature. Additional evaluation of the outcomes of sport participation (as distinct from physical activity) and the mechanisms through which these positive health outcomes are achieved is needed.
A promising line of research contends that positive outcomes of sport, including enhanced health and well-being, are achieved as a result of the ensuing sense of community that develops in and around sport settings.14-16 Previous research has shown that increased sense of community has a positive impact on retention and satisfaction for sport participants,2,17,18sport event volunteers,19 fans,20,21youth sport parents,22 and referees.23-25 While the sport literature clearly supports the proposition that increased sense of community is positively associated with the sport experience and implies a link to overall health, the literature outside of sport provides evidence of a direct link between sense of community and improved health.
While sport has been recognized as one of the few remaining social institutions that builds community,17,22,26 and the existence of a sense of community can contribute to positive health outcomes, it is unknown whether sport programmes are better suited to this and more effective in achieving these ends than other leisure activities such as music or art.27 In order to examine the importance of sense of community and its association with sport and positive health outcomes, the following sections review the literature related to: (1) sense of community and health; (2) sense of community and sport; and (3) sport and health.
Sense of Community and Health
Sense of community has been defined as “community characteristics that lead to members feeling a sense of belonging, attachment, and shared faith and interest in common goals or values.”28 The importance of individuals experiencing a sense of community in terms of health is well-documented in the community psychology field. Hill29 asserted that structures fostering a strong psychological sense of community are likely to be similar to those which foster healthy outcomes; thus, promoting a sense of community among individuals could lessen the need for specific interventions to target health improvements. Research in the community psychology realm suggests that increases in one’s sense of community leads to positive health and lifestyle benefits, such as significantly less drug use,30,31 improved well-being,32-34and lower stress.35 In addition, the sociological literature points to the connection between a lack of community, or anomie, and many negative health-related consequences,15,16 including deviant behaviour36-39 and physical and mental health decrements.40,41
Additionally, it is widely accepted that increased sense of community improves health through the promotion of health-enhancing behaviours.42-44 For example, a strong social network, social capital, and social ties (i.e., fundamental components and the basis in which sense of community is felt) have been associated with lower mortality,45 increased leisure-time and physical activity,46 decreased binge drinking,47,48 improved perception of overall health,49 and positive health behaviour change.50 Thus, it is not surprising that, “health promoters are increasingly becoming involved in general ‘community strengthening’ programmes, which seek to create ‘health-enabling communities’, characterized by trust, mutual support and high levels of involvement in local community projects of mutual interest”.42(p255-256) In general, many want to assume and credit “sport” for fostering health outcomes, but it may be likely that healthier people seek out sport.51 In an effort to better understand the unique effects of sport and its potential contribution to health, it important to study and consider comparative social groups and their structures.
Sense of Community and Sport
Hill’s assessment of community, described above, served as the basis for Warner and colleagues’ grounded theory work on exploring sense of community in a sport setting.28,52,53 The result of this work was Warner and Dixon’s Sport and Sense of Community Theory,16 which theorized that Administrative Consideration, Common Interest, Competition, Equity in Administrative Decisions, Leadership Opportunities, Social Spaces, and Voluntary Action are the fundamental factors or community characteristics that are needed for a sense of community to be fostered among athletes. Perhaps not surprisingly, sport and sport programming have been credited with being a context in which community and a sense of community are developed. In fact, Berg and colleagues2(p29) pointed out that “hedonic rewards and social interaction (and the ensuing sense of community)” are two primary benefits that sport and physical activity participants seek. The extant sport management literature has assumed that the building of community in sport is a positive process and has implied positive health outcomes are being achieved via the created sense of community.17,28,52
Sport and Health
Berg and colleagues suggested that an acknowledgement of the association between sense of community and sport and sense of community and health would aid in efforts to utilize sport for public health purposes.2 Eime and colleagues’ work further supports this notion, as they found that the social nature of sport has been associated with a range of psychological and social health benefits.51 However, researchers have also argued that sport can promote unhealthy behaviours. For example, previous research has shown that athletes are more likely to binge drink,7,54 suffer from eating disorders,55,56 and report higher levels of anxiety.57,58 As well, it must be acknowledged that sports and recreation-related injuries are detrimental to one’s overall health.59,60 Thus, a clear gap in the literature exists with regard to whether or not greater sense of community is related to positive health outcomes and if so, whether this association holds true for athletes.
Present Study
Consequently, the purpose of this study is to further understand the association between the communities formed via a sport programme and health outcomes. In the collegiate realm, several scholars have compared athletes to members of social organisations (i.e., fraternities and sororities, also commonly referred to as Greek organisations). This comparison is often done because both groups are considered high-risk for problem alcohol use and other negative associated outcomes.61-64 In an effort to identify and determine the unique contributions of sport programming and sport participation on health, university club sport athletes were evaluated and compared to a non-sport social group. Specifically, we included university social organisations (i.e., fraternities and sororities) as the comparator group, given that such organisations are often credited with fostering a sense of community65,66 and are also thought to promote more risk-taking and unhealthy behaviours. The comparison between athletes in club sport programmes and members of university social organisations allows for empirical investigation of the relative advantages (or disadvantages) of sport involvement in delivering positive health outcomes. The following research questions were developed to explore these associations:
- RQ1: Do increased levels of sense of community fostered in social settings lead to positive health outcomes?
- RQ2: Is there a difference in the sense of community experienced by club sports athletes in comparison to university social organisations participants?
- RQ3: Are there differences in health outcomes experienced by sport club athletes compared to members of university social organisations?
- RQ4: Are there differences in health outcomes between club sport groups and members of university social organisations when controlling for sense of community?
METHODOLOGY
Participants
The sampling frame for the current study consisted of undergraduate students from a mid-sized university in the southeastern United States who participated in either university-sponsored club sports or social organisations (i.e., fraternities or sororities). All 3,614 students who were involved in either a club sport or social organisation at the university were invited to participate in the study. A total of 781 usable surveys were returned for a response rate of 21.6%. Of the surveys returned, 59% (n = 458) were from club sport athletes and 41% (n = 323) from members of a university social organisation.
Procedure
University administrators provided a list of email addresses for club sport and university social organisation members. Participants were sent an email invitation and a link to an online survey about their sport or social organisation experiences. The email described the purpose of the study, contact information, time required to fill out the questionnaire (10 to 20 minutes), and the participant’s right to refuse to complete the survey or stop responding at any time. No incentives to complete the survey were offered. Two follow up emails were sent to remind students to complete the survey.
Instrumentation
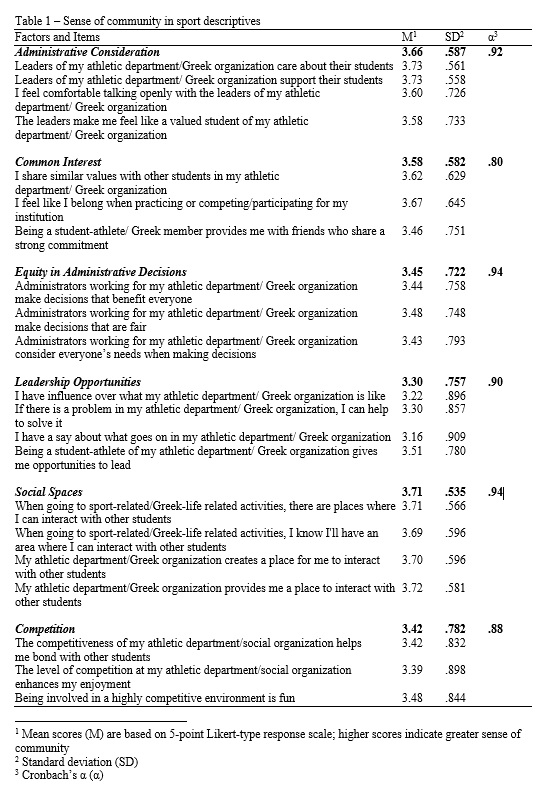
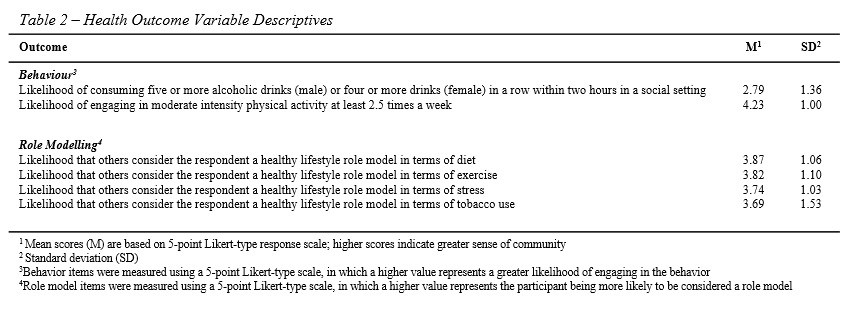
The survey consisted of three sections with a total of 31 items. The first section of the study contained a 21-item Sense of Community in Sport Scale (SCS).18 The SCS consists of 6 Subscales (Administrative Consideration, Common Interest, Equity in Administrative Decisions, Leadership Opportunities, Social Spaces, and Competition), measured on 5-point Likert-type scales. The SCS measure has shown satisfactory reliability and validity in previous research with Cronbach’s alpha scores ranging from .76 to .86 and Average Variance Extracted (AVE) scores ranging from .62 to .72 for each sub-dimension.18 Higher scores indicate a greater sense of community. Table 1 provides an overview of the SCS scale with all sub-dimensions and individual items listed. The second section of the survey consisted of six items related to participants’ overall well-being and healthy lifestyle choices. Two items asked respondents to provide information on the frequency with which they engage in specific health behaviours – one positive (i.e., physical activity) and one negative (i.e., binge drinking). These items specifically asked “How likely are you to engage in moderate intensity physical activity at least 2.5 hours a week?” and “How likely are you to consume five or more alcoholic drinks (males) or four or more drinks (females) in a row within two hours at a social outing?” These items are based on the National Institute of Health recommended physical activity guidelines and definition of binge drinking. Four additional items measured how likely respondents were to believe that others considered them a role model in terms of diet, exercise, stress management, and tobacco use. Social support has been determined to be an important factor in the promotion of positive health behaviours; consequently, the study used role model items as a complement to the behavioural items above. These were all single-item measures examined through 5-point Likert-type scales. Table 1 provides descriptive information for the SCS and Table 2 provides descriptive information on well-being and healthy lifestyle choice outcomes. The final section of the survey contained four demographic questions examining respondents’ gender, race, academic status, and grade point average (GPA).
Data Analysis
Preliminary analyses were conducted on continuous variables to assess normality. All continuous variables used in the examination were found to be normally distributed. Preliminary analyses were also conducted on the SCS to provide reliability-related evidence. Reliability-related evidence was provided for each sub-dimension of the SCS, with Cronbach’s alpha scores ranging from .80 to .94 for each sub-dimension of the SCS (See Table 1).
To address RQ1, six multiple regression models were developed to examine the impact of sense of community sub-dimensions on positive health outcomes. The first two regression models contained dependent variables focused on health-related behaviours (physical activity and binge drinking). The final four regression models contained dependent variables focused on role modelling (diet, exercise, stress, and tobacco usage). Independent variables were the same for all regression models and included all six SOC sub-dimensions. For RQ2, an independent samples t-test was developed to examine group differences in sense of community experienced between club sports athletes and social organisation participants. For RQ3 and RQ4, six ANCOVA models were developed to examine group differences in health outcomes between sport club athletes and members of social organisations, controlling for sense of community.
RESULTS
Demographics
Of the 781 respondents, 56.4% were female and 74.6% were Caucasian (followed by 7.3% African-American). Respondents were similarly distributed across academic class. Most respondents were freshman (24.5%), followed closely by sophomores (22.9%) and seniors (21.6%). The average GPA for respondents was 3.17 (SD = .657) on a 4.0 GPA scale. Results indicated comparable demographic percentiles between study participants and the general population of undergraduate students at the institution with respect to gender (58% female), race (69.3% Caucasian), class (27.0% freshman), and GPA (3.0).
Sense of Community and Health Outcomes
In the first two regression models focusing on lifestyle habits in relation to sense of community (RQ1), the physical activity model was significant F(6,717) = 11.55, p < .001 (Table 3). However, the sense of community sub-dimensions only explained 8.8% of the variance in physical activity choices. Common Interest (p = .003), Equity in Administrative Decisions (p = .007), and Competition (p < .001) significantly influenced physical activity. The binge drinking model was not found to be significant.
In the next four regression models focused on role model perceptions related to healthy living, the diet model was significant F(6,720) = 7.18, p < .001. However, the sense of community sub-dimensions only explained 5.6% of the variance in healthy eating habits. Social Spaces (p = .001) and Competition (p = .009) significantly influenced diet. The exercise model was significant F(6,720) = 5.94, p < .001. However, the sense of community sub-dimensions only explained 4.7% of the variance in exercise. Competition (p < .001) was the only sub-dimension that significantly influenced exercise. The stress model was significant F(6,720) = 7.09, p < .001. However, the sense of community sub-dimensions only explained 5.6% of the variance in healthy eating habits. Leadership Opportunities (p = .001) was the only sub-dimension that significantly influenced stress. The tobacco use model was not found to be significant.
Sense of Community and Organisation Affiliation
Participants in club sports showed a higher sense of community (M = 75.17, SD = 10.158) than participants in social organisations (M = 72.17, SD = 12.134). The results of the independent samples t-test were significant (t(781) = -3.628, p < .001) (not pictured).
Health Outcomes and Organisation Affiliation
The first two ANCOVA models examined differences between groups in lifestyle habits when controlling for overall sense of community (RQ3 and RQ4) (Table 4). There was a significant effect of organisational affiliation on binge drinking after controlling for sense of community, F(1,721) = 9.84, p = .002, η2 = .013 (Table 4). Respondents affiliated with social organisations were more likely to binge drink (M = 2.99, SD = 1.32) than respondents affiliated with club sports (M = 2.66, SD = 1.37). There was also a significant effect of organisational affiliation on physical activity after controlling for sense of community, F(1,721) = 126.93, p = < .001, η2 = .150, but in the opposite direction. Respondents affiliated with club sports were more likely to participate in physical activity (M = 4.56, SD = .756) than respondents affiliated with social organisations (M = 3.73, SD = 1.13).
In the four ANCOVA models focused on role model perceptions related to healthy living, after controlling for sense of community, there was a significant difference in role model perceptions of diet F(1,724) = 144.79, p = < .001, η2 = .185, exercise F(1,724) = 61.43, p < .001, η2 = .078, and tobacco usage F(1,724) = 17.84, p < .001, η2 = .024 based on organisational affiliation. Club sports respondents were more likely to consider themselves role models in terms of healthy living compared to social organisation respondents. Group differences related to stress were not found to be significant.


DISCUSSION
The results of the current research provide limited support for the positive influence of a sense of community on health outcomes (RQ1), while providing preliminary evidence of differences in sense of community (RQ2) and health outcomes (RQ3) when sport and non-sport participants are compared. Regarding RQ1, the finding that very little variance in the health outcomes was explained by participants’ sense of community is likely a result of both groups reporting high levels of sense of community (RQ4). This finding is not surprising, because decisions related to various health behaviours are complex and influenced by a variety of individual and environmental factors. Still, sense of community did contribute to positive health outcomes for four of the six health behaviours and role modelling variables: frequency of physical activity, and being a role model for diet, exercise, and stress. Thus, these findings suggest that individuals who reported a stronger sense of community also were more likely to adhere to pro-social health behaviours. This finding is reinforced by the Social Support Model in public health, which stresses the importance of personal support and relationships in maintaining health.40,50,67 This finding is noteworthy for sport managers concerned with improving health for participants. That is, the results suggest that health can be improved through enhancing the sense of community experienced by sport participants.
The importance and practical implications of the findings regarding the influence of sense of community on health outcomes can be found by examining the specific factors that were significant. Higher levels of competition, which is defined as the challenge to succeed against internal and external rivalries, led to individuals being more likely to engage in physical activity 2.5 hours per week and more likely to believe that others considered them role models in terms of diet and exercise. Individuals who believe competition is enjoyable, fun, and helps with group bonding may choose to “compete” on the basis of physical activity and its benefits (e.g., improved athletic performance, physical attractiveness). Further, these individuals may also be motivated to compete or stand out from the crowd by being a role model (i.e., not only do they want to engage in the behaviour, but they want to be seen by their peers as being the best at these behaviours). This finding is not surprising given that competition is so deeply imbedded in Western society and has been found to be a factor that can lead to participant retention.68.69 Thus, emphasizing competition may be one way sport managers can help improve health behaviours of participants.
Common Interest, which brings together individuals and influences group dynamics, social networking, and friendships, was also a significant predictor of physical activity. Physical activity can have a social component, and in fact, the social nature of physical activity participation may even aid in maintenance of a physical activity programme.2.70 Thus, individuals who indicate high levels of common interest may seek the social benefits associated with engaging in physical activity with their peers. Finally, the finding that Social Spaces were significant for the diet variable may be explained by the powerful influence of social norms.71,72 Individuals who have opportunities to interact with peers in a shared common area or facility may feel positive pressure to engage in healthy eating behaviours and model them. Overall, the power of a sport environment to impact health should not be overlooked.27,73 This work demonstrates the importance of community characteristics typically and perhaps, even organically, found in sport settings that can contribute to positive health outcomes.
Turning to RQ2, both participants in club sport and participants in university social organisations exhibited high levels of sense of community. However, when the sense of community of participants in social organisations and club sport are compared, significant differences were observed. Club sport is largely student organized and run, which could explain club sport participants’ higher reported sense of community. While university social organisations are student-led to an extent, they also have hierarchical structures (absent in club sport) in which the national office of a fraternity or sorority may be deemed geographically and culturally distant. In addition, sense of community could be explained by the centrality of sport to an individual who continues participation through college. By this point, individuals could have spent fifteen or more years participating in organized sport. For social organisation participants, there is not necessarily a clear common activity that brought members together. Identification as a member of the university social organisation is first available in college, so the length of time an individual is associated with their organisation may explain the observed differences.
Regarding RQ3, our results demonstrated that although members of both university social organisations and club sport had relatively high levels of sense of community, significant differences were observed in the health outcomes between the two groups. Participants in club sport exhibited more desirable health behaviours than university social organisation participants across all variables studied. This finding contradicts previous research that considers both sport participants and participants in university social organisations to be at high-risk for negative health outcomes.61-64 This also is consistent with the Health through Sport model that demonstrates a relationship between psychological, psychosocial, and social health domains and sport participation,51,74 and lends support to Eime and colleagues’ suggestion that the social nature of sport can influence the extent to which health benefits are realized.51 This work supports the potential of community engagement through sport to promote positive health outcomes. Further, the results of this study suggest that rather than promoting risky behaviours,62,64,75 the organisational structures of sport may, in fact, promote healthy behaviours. This result is consistent with previously untested claims found in the sport management literature.2,4,5,51 Sport participants typically place a higher priority on health, which affects athletic performance. There are practical implications for universities. University social organisations and campus recreation (which typically includes oversight for club sport) are commonly units of the same department (e.g., Student Life, Student Affairs) and competing for the same resources. If club sports are better able to deliver health benefits to students, campus recreation staff can make compelling arguments for increased financial support from the university. Although this research took place in a university setting in a developed country, any sport-for development initiative that seeks ways to secure funding can also benefit from these findings.76 Moreover, sense of community likely plays an even bigger role in disadvantaged communities where the majority of sport for development programmes target. Since “one of the biggest challenges for disadvantaged people is to find a community with which to identify and belong”77(p255) understanding the positive influence of sense of community on health-related outcomes in other sport for development settings may even be stronger.
While the results of this research suggest the nature of the association between sport participation and health outcomes, there are limitations that need to be acknowledged. Specifically, it is possible that sport club members are better informed about healthy lifestyles than their counterparts in social organisations, which could result in a response bias (i.e., self-report of more desirable health behaviours from sport club participants). Additionally, it is possible that individuals who are more concerned with their health would choose to participate in a sport club rather than in a university social organisation, and this would raise issues of selection bias.
Future research should add sense of community to the many established factors in the extant literature to develop a regression model that accounts for a greater degree of variance in the model. This work represents the first use of the SCS scale for non-athlete populations. Future research should also consider extending the use of this tool to other populations in various other sport for development settings and outside of sport, such as local social and community groups. While the response rates in this study were comparable to those found in sport management research and the demographics of the sample were comparable to the demographics of the student body, results of this study cannot be generalized beyond the participants surveyed. Additionally, expanding the study such that more individuals with lower sense of community are surveyed would shed further light on the issues examined.
CONCLUSION
Sport organisations have the opportunity to contribute to public health and positive health outcomes. This study empirically tested the associations that have led researchers and practitioners to make claims about the association between sport and health. Specifically, limited support was found for the following associations: (1) sport participation can influence individual’s sense of community; (2) sport participation can influence health outcomes; and (3) the development of sense of community can impact the extent to which health outcomes are achieved by sport participants. An additional contribution of this research is the use of a comparison group in a university setting to examine whether sport participation is more effective than university social organisations in developing sense of community and promoting health behaviours. This research provides empirical evidence for sport managers to consider, strengthen and ultimately better position sport such that it positively contributes to health.
REFERENCES
1. World Health Organization. WHO Definition of health [Internet]. 2003. Available from: http://www.who.int/ about/definition/en/print.html
2. Berg BK, Warner S, Das BM. What about sport? A public health perspective on leisure-time physical activity. Sport Manag Rev. 2015 Feb;18(1):20–31.
3. Dalton B, Wilson R, Evans JR, Cochrane S. Australian Indigenous youth’s participation in sport and associated health outcomes: Empirical analysis and implications. Sport Manag Rev. 2015;18(1):57–68.
4. Gallant D, Sherry E, Nicholson M. Recreation or rehabilitation? Managing sport for development programs with prison populations. Sport Manag Rev. 2015;18(1):45–56.
5. Rowe K, Shilbury D, Ferkins L, Hinckson E. Sport development and physical activity promotion: An integrated model to enhance collaboration and understanding. Sport Manag Rev. 2013;16:364–77.
6. Sefiha O. Bad Sports: Explaining sport related deviance: Bad sports: Explaining sport related deviance. Sociol Compass. 2012 Dec;6(12):949–61.
7. Lisha NE, Sussman S. Relationship of high school and college sports participation with alcohol, tobacco, and illicit drug use: A review. Addict Behav. 2010 May;35(5):399–407.
8. Wichstrøm T, Wichstrøm L. Does sports participation during adolescence prevent later alcohol, tobacco and cannabis use? Addiction. 2009 Jan;104(1):138–49.
9. U.S. Department of Health and Human Services, Public Health Service [Internet]. Office of the Surgeon General; 2010. Available from: http://www.surgeongeneral.gov/ library/obesityvision/obesityvision2010.pdf
10. U.S. Department of Health and Human Services. Healthy People 2020 2013 Healthy People [Internet]. 2013;2020. Available from: http://www.healthypeople.gov /2020/topicsobjectives2020/objectiveslist.aspx?topicId=33
11. Brownson RC, Boehmer TK, Luke DA. Declining rates of physical activity in the United States.: What are the contributors? Annu Rev Public Health. 2005 Apr 21;26(1):421–43.
12. Edwards MB. The role of sport in community capacity building: An examination of sport for development research and practice. Sport Manag 2015;18(1):6–19.
13. Lyras A, Welty Peachey J. Integrating sport-for-development theory and praxis. Sport Manag Rev. 2011 Nov;14(4):311–26.
14. Swyers H. Wrigley Regulars: Finding community in the bleachers?, University of Illinois Press: Champaign. IL; 2010.
15. Warner S. Sport and Community. In: Cunningham GB, Singer JN, editors. Sociology of sport and physical activity. 2nd ed. College Station, TX: Center for Sport Management Research and Education; 2012. p. 237–54.
16. Warner S. Sport and Sense of Community Theory. In: Cunningham GB, Fink J, Doherty A, editors. Routledge handbook of theory in sport management. New York, NY: Routledge; 2016. p. 189–98.
17. Warner S, Leierer S. Building community via sport for adolescents. J Appl Sport Manag. 2015;4:84–102.
18. Warner S, Kerwin S, Walker M. Examining sense of community in sport: Developing the multidimensional “SCS”Scale. J Sport Manag. 2013;27(5):349–62.
19. Kerwin S, Warner S, Walker M, Stevens J. Exploring sense of community among small-scale sport event volunteers. Eur Sport Manag Q. 2015 Jan;15(1):77–92.
20. Fairley S, Tyler B. Bringing baseball to the big screen: Building sense of community outside of the ballpark. J Sport Manag. 2012;26:258–70.
21. Warner S, Shapiro S, Dixon MA, Ridinger LL, Harrison S. The football factor: Shaping community on campus. J Issues Intercoll Athl. 2011;4:236–56.
22. Warner S, Dixon M, Leierer S. Using youth sport to enhance parents’ sense of community. J Appl Sport Manag. 2015;7:45–67.
23. Kellett P, Warner S. Creating communities that lead to retention: The social worlds and communities of umpires. Eur Sport Manag Q. 2011 Dec;11(5):471–94.
24. Warner S, Tingle J, Kellett P. Officiating attrition: The experiences of former referees. J Sport Manag. 2013;27:316–28.
25. Tingle JK, Warner S, Sartore-Baldwin ML. The Experience of former women officials and the impact on the sporting community. Sex Roles. 2014 Jul;71(1-2):7–20.
26. Armstrong G, Giulianotti R. Entering the field: New perspectives on world football. Oxford: Berg; 1997.
27. Green BC. Sport as an agent for social and personal change. In: Girginov V, editor. Management of Sports Development. London: Butterworth-Heinemann; 2008. p. 131–47.
28. Warner S, Dixon MA. Understanding sense of community from the athlete’s perspective. J Sport Manag. 2011;25(3):257–71.
29. Hill J. Psychological sense of community: Suggestions for future research. J Community Psychol. 1996;24:431–8.
30. Battistich V, Hom A. The relationship between students’ sense of their school as a community and their involvement in problem behaviors. Am J Public Health. 1997;87(12):1997–2001.
31. Mayberry ML, Espelage DL, Koenig B. Multilevel modelling of direct effects and interactions of peers, parents, school, and community influences on adolescent substance use. J Youth Adolesc. 2009 Sep;38(8):1038–49.
32. Kutek SM, Turnbull D, Fairweather-Schmidt AK. Rural men’s subjective well-being and the role of social support and sense of community: Evidence for the potential benefit of enhancing informal networks: Rural men’s well-being and social support. Aust J Rural Health. 2011 Feb;19(1):20–6.
33. Albanesi C, Cicognani E, Zani B. Sense of community, civic engagement and social well-being in Italian adolescents. J Community Appl Soc Psychol. 2007 Sep;17(5):387–406.
34. Jose PE, Ryan N, Pryor J. Does social connectedness promote a greater sense of well-being in adolescence over time? J Res Adolesc. 2012 Jun;22(2):235–51.
35. Young AF, Russell A, Powers JR. The sense of belonging to a neighbourhood: Can it be measured and is it related to health and well being in older women? Soc Sci Med. 2004 Dec;59(12):2627–37.
36. Agnew R. The nature and determinants of strain: Another look at Durkheim and Merton. In: The future of Anomie Theory. 1997.
37. Carter EM, Carter MV. Social psychological analysis of anomie among National Football League players. Int Rev Sociol Sport. 2007;42:243–70.
38. Hagan J, McCarthy B. Anomie, social capital, and street criminology. In: Passas N, Agnew R, editors. The future of Anomie Theory. Boston: Northeastern University Press; 1997. p. 124–41.
39. Hirschi T. Causes of delinquency. Berkeley: University of California Press; 1969.
40. Berkman LF, Glass T, Brissette I, Seeman TE. From social integration to health: Durkheim in the new millennium. Soc Sci Med. 2000;51:843–57.
41. Deflem M. From anomie to anomia and anomic depression: A sociological critique on the use of anomie in psychiatric research. Soc Sci Med. 1989 Jan;29(5):627–34.
42. Campbell C, Jovchelovitch S. Health, community and development: Towards a social psychology of participation. J Community Appl Soc Psychol. 2000 Jul;10(4):255–70.
43. Durkheim E. Suicide: A study in sociology translated by George Simpson and John A. New York: The Free Press; 1951.
44. McMillan D, Chavis D. Sense of community: A definition and theory. J Community Psychol. 1986;14:6–23.
45. Kawachi I, Kennedy BP, Lochner K, Prothrow-Stith D. Social capital, income inequality, and mortality. Am J Public Health. 1997 Sep;87(9):1491–8.
46. Lindström M, Hanson BS, Östergren P-O. Socioeconomic differences in leisure-time physical activity: The role of social participation and social capital in shaping health related behaviour. Soc Sci Med. 2001 Feb;52(3):441–51.
47. Weitzman ER, Chen YY. Risk modifying effect of social capital on measures of heavy alcohol consumption, alcohol abuse, harms, and secondhand effects: National survey findings. J Epidemiol Community Health. 2005;59(4):303–9.
48. Weitzman ER, Kawachi Giving means receiving: The protective effect of social capital on binge drinking on college campuses. Am J Public Health. 1936;90.
49. Ross N. Community belonging and health. Health Rep. 2001;13(3):33–9.
50. Hystad P, Carpiano RM. Sense of community-belonging and health-behaviour change in Canada. J Epidemiol Community Health. 2012 Mar 1;66(3):277–83.
51. Eime R, Young JA, Harvey JT, Charity MJ, Payne WR. A systematic review of the psychological and social benefits of participation in sport for children and adolescents: Informing development of a conceptual model of health through sport. Int J Behav Nutr Phys Act. 2013;10(1):98.
52. Warner S, Dixon MA, Chalip LC. The impact of formal versus informal sport: Mapping the differences in sense of community. J Community Psychol. 2012;40:983–1003.
53. Warner S, Dixon MA. Sports and community on campus: Constructing a sports experience that matters. J Coll Stud Dev. 2013;54(3):283–98.
54. Martens MP, Watson JC, Beck NC. Sport-type differences in alcohol use among intercollegiate athletes. J Appl Sport Psychol. 2006 Jul;18(2):136–50.
55. Martinsen M, Sundgot-Borgen J. Higher prevalence of eating disorders among adolescent elite athletes than controls. Med Sci Sports Exerc. 2013;45(6):1188–97.
56. Smolak L, Murnen SK, Ruble AE. Female athletes and eating problems: A meta-analysis. Int J Eat Disord. 2000;27:371–80.
57. Huffman LT. Examining perceived life stress factors among intercollegiate athletes: A holistic perspective (doctoral dissertation). University of Tennessee; 2014.
58. Kimball A, Freysinger VJ. Leisure, stress, and coping: The sport participation of collegiate student-athletes. Leis Sci. 2003;115–41.
59. Oates W. An injury prevention curriculum for coaches [Internet]. 2011. Available from: http://media.hometeams online.com/photos/baseball/MISSOURICHARGERS/Coaches_Curriculum_Preventing_Injury_Winter_2011.pdf
60. Rechel JA, Yard EE, Comstock RD. An epidemiologic comparison of high school sports injuries sustained in practice and competition. J Athl Train. 2008 Mar;43(2):197–204.
61. Foubert JD, Perry BC. Creating lasting attitude and behavior change in fraternity members and male student athletes: The qualitative impact of an empathy-based rape prevention program. Violence Women. 2007 Jan 1;13(1):70–86.
62. Thompson K, Hein E. Postcollege Criminal Convictions: A comparison of Greek, athlete, and other student offending. J Coll Character [Internet]. 2014 Jan 1 [cited 2016 Apr 13];15(4). Available from: http://www.tandfonline.com/doi/full/10.1515/jcc-2014-0028
63. Turrisi R, Mallett KA, Mastroleo NR, Larimer ME. Heavy drinking in college students: Who is at risk and what is being done about it? J Gen Psychol. 2006 Oct;133(4):401–20.
64. Huchting KK, Lac A, Hummer JF, LaBrie JW. Comparing Greek-affiliated students and student athletes: An examination of the behavior-intention link, reasons for drinking, and alcohol-related consequences. J Alcohol Drug Educ. 2011 Dec 1;55(3):61–81.
65. DeBard R, Lake T, Binder RS. Greeks and Grades: The first-year experience. NASPA J [Internet]. 2006 Jan 10 [cited 2016 Jul 26];43(1). Available from: http://www.degruyter.com/view/j/jsarp.2006.43.issue-1/jsarp.2006.43.1.1571/jsarp.2006.43.1.1571.xml
66. Lounsbury JW, DeNeui D. Psychological sense of community on campus. Coll Stud J. 1995
67. Henderson KA. A paradox of sport management and physical activity interventions. Sport Manag Rev. 2009 May;12(2):57–65.
68. Kohn, A. (1986). No contest: The case against competition. Boston: Houghton Mifflin, 257 pp., $16.95. Psychol Sch. 1991 Apr;28(2):182–3.
69. Warner S, Dixon MA. Competition, gender and the sport experience: An exploration among college athletes. Sport Educ Soc. 2015 May 19;20(4):527–45.
70. Sherwood NE, Jeffery RW. The behavioral determinants of exercise: Implications for physical activity interventions. Annu Rev Nutr. 2000;20.
71. Ball K, Jeffery RW, Abbott G, McNaughton SA, Crawford D. Is healthy behavior contagious: Associations of social norms with physical activity and healthy eating. Int J Behav Nutr Phys Act. 2010;7(86.).
72. Reid AE, Cialdini RB, Aiken LS. Social norms and health behavior. In: Handbook of behavioral medicine. 2010. p. 263–74.
73. Inoue Y, Berg BK, Chelladurai P. Spectator sport and population health: A scoping study. J Sport Manag. 2015 Nov 1;29(6):705–25.
74. Casey M, Eime R. Sport and Health. In: Bowers MT, Dixon MA, editors. Sport management: An exploration of the field and its value. 1st ed. Urbana, IL: Sagamore; 2015. p. 61–86.
75. Worthen MGF. Blaming the jocks and the Greeks?: Exploring collegiate athletes’ and fraternity/sorority members’ attitudes toward LGBT individuals. J Coll Stud Dev. 2014;55(2):168–95.
76. Kidd B. A new social movement: Sport for development and peace. Sport Soc. 2008 Jul;11(4):370–80.
77. Skinner J, Zakus DH, Cowell J. Development through sport: Building social capital in disadvantaged communities. Sport Manag Rev. 2008 Nov;11(3):253–75.
