1 Obafemi Awolowo University, Department of Physical and Health Education, Nigeria
Citation: Obadiora, A.H. The influence of sport participation on quality of life perceptions among inmates in Nigerian prisons. Journal of Sport for Development. 2016; 4(6): 36-43.
Abstract
The purpose of this study was to investigate the effects of participation in football activities on quality of life perception among randomized inmates of Nigerian prisons, in Ile-Ife and Ilesa in Osun State, Nigeria. The study participants were 180 inmates of Ilesa and Ile-Ife Prisons in Osun State, Nigeria who are within the ages of 21 to 35 years old. Each participant was selected and randomly assigned to experimental (n=90) or control subjects (n=90). The subjects were administered with pre-test instruments through the football participation assessment and Quality of Life (QOL) test after which only subjects in experimental groups participated in football sessions for a period of eight weeks. Subsequently, all respondents were administered with post-test instruments (football proficiency self-assessment, game experience and QOL tests). QOL was measured using the adapted version of World Health Organization’s Quality of Life- Bref (WHOQOL-BREF). Results show that inmates who participated in football activities have higher general quality of life perception than those who did not. However, social wellbeing is improved for both active and passive (spectators) participants. Sport skills acquisition and participation positively affect physical health, psychological and social wellbeing of inmates. Participation therefore affects the general QOL of inmates of Federal prisons in Osun State, Nigeria.
Introduction
There is widespread consensus about the positive relationship between sport participation and health. Research evidences illustrate that physical activity and sports positively affect psychological and mental health conditions such as anxiety, depression, mood and emotion, self-esteem and psychological dysfunction.1 It has further been discovered that engagement in sport and physical activities offers a multitude of benefits, including enhanced physical fitness, increased social support networks, elevated positive affective states, and the development of perceptions of competence and enjoyment.2 Contrasting inactivity and enhancing well-being is usually the first reason given when encouraging sports activities; indeed, there is a large body of literature showing that inactivity is one of the most significant causes of death, disability and reduced quality of life.3 Given these benefits, there is a potential for the development of positive psychological growth through sport and physical activity. For these reasons, sport and physical activity participation has been recommended as a way to enhance overall quality of life in various populations.2-6 There has been, unfortunately, limited empirical research focused on understanding how sport and physical activity impacts physical, social and mental health among inmates undergoing correctional and rehabilitation processes in Nigerian prisons. There are, however, research that suggests that stress and coping strategies, social support and general emotional experiences may lead to positive psychological outcomes associated with confinement.7-11 It has also been observed that physical activity and QOL relationship is positive and consistent across subgroups, activity settings, and activity mode.12 Prison inmates are important target population for sport activities, since imprisonment is associated with psychological distress, anxiety and poor overall quality of life.9-11
Sports and Quality of Life of General Population
According to findings from a study of community integration, recreational sport for the general population brings about a positive relationship among all four of the domains of QOL, which are physical, psychological, social and environmental.13 Specifically, football was observed to facilitate compliance and contribute to maintenance of a socially and physically active lifestyle. It was believed that structured football participation for two to three hours per week causes significant cardiovascular, metabolic and musculoskeletal adaptations, independent from gender, age or one’s lack of experience. Individuals who played football were also observed to develop high levels of social interaction and overall flow during the period of active participation, which underlines that they felt motivated, happy and involved to the point where they forgot time and fatigue.14
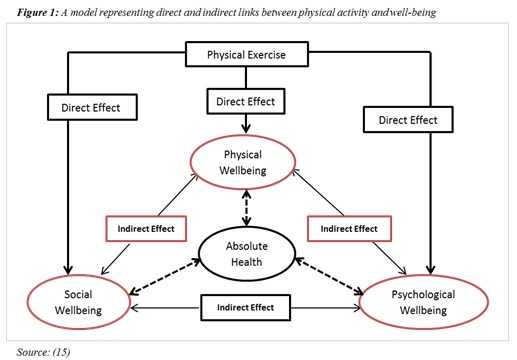
Most previous researchers on effects of sports and physical activities on well-being expressed models to explain the interaction effects of sports skills and participation on quality of life. These conceptual frameworks explained indirect interaction effects of each of the components of quality of life such as social, psychological and physical wellbeing on each other.15-16 The model presented in the diagram below forms the significant foundation for this study.
Purpose of Study
It has been shown through various studies that participation in physical activities and sports can improve social, physical, mental and psychological health of convalescent patients, adolescents, youth and aged persons. Many studies have also shown that sport activities can improve the self-reported QOL perception of the general population. Little of the research focuses on prison inmates despite the fact that inmates suffer more from poor physical health and low quality of life. The few studies of the effects of physical activities on QOL of prison inmates were done in developed countries where the prison services observe at least the minimum standard for promoting inmate welfare. Resource-poor prisons in developing countries such as those in Nigeria differ markedly from prisons in developed countries. Therefore, the purpose of this study was to investigate the effect of sport (i.e. football) skills acquisition and participation on the quality of life (QOL) of inmates of Ilesa and Ile-Ife prison yards in Osun State, Nigeria.
Hypothesis
Football participation will not have significant effects on the quality of life (physical health, psychological and social well-being) perception by inmates of Nigeria Prisons.
Methods
Participants
The study took place through an experimental design. Inmates of Ilesa and Ile-Ife prison yards in Osun State, Nigeria were the population for the study. The study methodology was approved by the Department of Physical Education of the Obafemi Awolowo University and the Osun State Command of Nigerian Prison Service (NPS). The researcher engaged four research assistants including two prison officers who assisted the researcher during the administration of the study instruments and sports participation. Willingness to participate (WTP) in the study is 97.2% with a total of 380 out of 391 inmates who were both qualified (between age 20 and 35 years) and volunteered to participate in the study. The 97.2% WTP rate by qualified inmates eliminates possible bias in the self-selection method. The participants were informed about the purpose and methods of the study. They were also informed that their participation in the study is voluntary. This information was considered necessary to enable the respondents to make informed decision to accept or reject their participation in the study. Thereafter, they were asked to complete and sign an informed consent form containing the purpose, descriptions and possible discomforts or risks of the study along with the right of respondents to withdraw their continued participation at any time if they so desired. Open and random selection of 180 respondents for the study was done in the prison playing grounds. 90 participants selected from each of the two prison yards were further randomized to experimental (n=45) and control (n=45) groups respectively. Those selected among the inmates who volunteered for the study were those between the age range of 20 and 35 years old because young adulthood typically covers the period from 20-35 years of age, when both biological function and physical performance reach their peak.18 Inmates who were certified as medically or mentally unfit by the prisons’ welfare officers were excluded from the study.
Procedure
The study’s duration was 10 weeks. The first week was used for the administration of the research instrument to all of the respondents (n=180) and training of participants in experimental group (n=90) on the theory of football including rules and regulations of the games. The study instrument consists of Football Participation Test (FPT) and Quality of Life (QOL) questionnaire. Their scores were recorded as pre-test scores accordingly. Subsequently, only the respondents in experimental groups were further randomized into 10 teams of nine players. Each team ensured the active participation of all of the members of the experimental group during football participation sessions, which were held weekly for a period of eight weeks. Mental skill training was integrated into the football practice and participation sessions as individual subjects and teams were made to set goals for sport achievement. The steps followed during the goal setting include the following: evaluation of players’ current skill and participation experience level; setting of goals to be achieved by individual player or team within the available time; determination of individual or team strengths; determination of skill areas that need development; prioritisation of participant’s skill needs and selection of Two or Three Goals.17, 19 These goals include short-term and long-term goals (e.g. dribbling skills, endurance fitness and winning the tournament) and setting hard but realistic goals, including a timeline for achievement. Participants or teams also outlined strategy for achieving and evaluating progress every week and few minutes before football sessions.
The study adopted double round robin or league method for football tournament among the experimental subjects to provide subjects with ample opportunities for active participation during football participation session and not for the purpose of separate data analysis. After eight weeks of football participation session, all the respondents in control group (n=90) and experimental group (n=90) were administered with the FPT and QOL questionnaires. The scores were recorded as post-test scores accordingly.
Study Instrument
For the purpose of this study, a self-reported football participation assessment questionnaire was developed for respondents to separately rank their proficiency (passing, shooting, dribbling, tackling) and previous game experience (leisure or past-time, non-formal competitions, formal competitions) between 1 and 5. QOL perceptions of respondents were measured using the World Health Organization Quality of Life- Bref (WHOQOL-BREF) scale, which is a self-reported questionnaire that contains 26 items where each item represents 1 facet. The facets are defined as those aspects of life that are considered to have contributed to a person’s QOL. The WHOQOL-Bref contains 26 items, 24 of them make up the 4 domains of physical health (7 items), psychological health (6 items), social relationships (3 items), and environment (8 items); the other remaining 2 items measure overall wellbeing. WHOQOL instrument’s validity and reliability has been tested through various research and pilot studies and observed to be capable of discriminating between good and poor health along with general QOL.20-25 Nigeria studies also showed similar findings.20,26,27
Data Analysis
Data collected from the two selected prisons were merged and entered to SPSS format using version 15.0. Mean scores were analysed with descriptive and inferential statistics to determine whether differences observed in QOL measurements between the control and experimental groups are significant and can be attributed to football participation. The result was tested with regression analysis. A minimum level of significance of p < 0.05 was used as the entry requirement.
Results
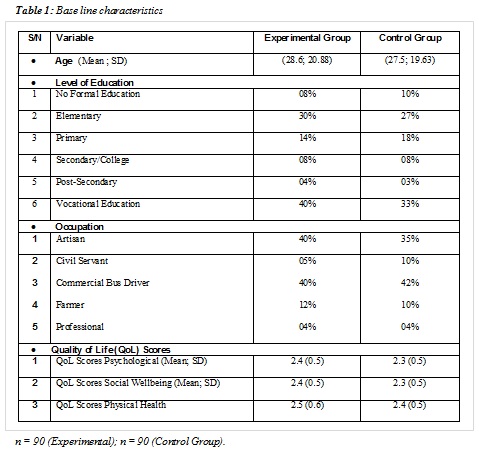
Socio-demographic characteristics were similar across the study groups at baseline (Table 1). While the mean age for the experimental group was 28.6 years, it was 27.5 years for that of the control group. Although those in the experimental arm were slightly more likely to be artisan and famers with lower educational levels, potentially more important are the higher proportions of participants in the experimental group reporting to have vocational education than the control group (Table 1). Furthermore, findings revealed some slight significant differences between the arms in baseline sport participation scores. Findings in baseline characteristics raise concerns about differential consent across the groups in terms of perceived quality of life. These are presented in Table 2 and Table 3.
At the end of the sport period, a proportion in the experimental group reported a higher QoL than in the control arm (Table 2). Although, the absolute difference and the (unadjusted) odds ratio were sizeable, however, there was evidence of a difference beyond chance (p=0.067). From the unadjusted figures, the adjustment of the variables related to consent and/or exhibiting any suggestion of baseline imbalance had only a minimal impact on the odds ratio and confidence interval. Likewise, imputing missing values had effect on the results. For instance, the unadjusted results changed to an odds ratio of 0.56 (95% CI 0.29, 1.09), p=0.086.
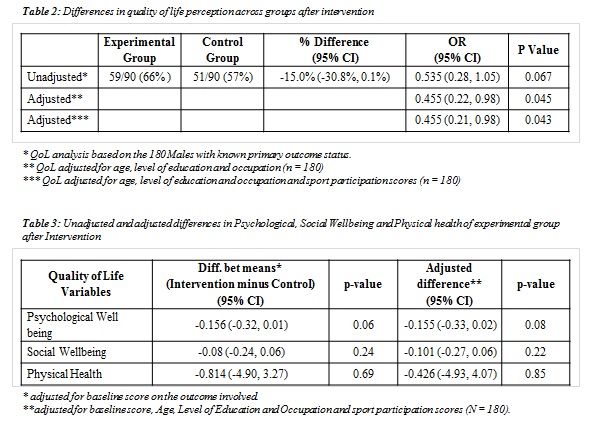
For the outcomes at the end of sport participation, there was evidence of a beneficial effect of the intervention (Table 3), predominantly on inmates’ psychological score. Again, imputing missing outcome data had an appreciable effect on these results. Consenting participants in the experimental group were assigned to one of the football teams (average of 15 per team). Adjusting for clustering by the experimental group had very little impact on any of the training prior to the primary outcome being ascertained, while 65% of participants in the experimental group attended at least six sessions of sport tournaments. From the instrumental variables regression analyses, the QoL was increased in absolute terms by 2.4 percentage points for each session attended (95% CI -4.9%, 0.0%, p=0.049). Introducing interaction terms between the control group and age factors, psychological and social wellbeing provided evidence of differential effects of the sport participation on QoL (p values of 0.83, 0.19 and 0.43 respectively).
There was evidence of a beneficial effect of the sport participation in terms of reducing inmate psychological anxiety and enhancing social wellbeing at the end of their soccer participation sessions. The confidence intervals rule out any important deleterious effects of the sport participation but the precision attained leaves equivocal results as to whether there is an important benefit from the sport participation. A reduction of fifteen percentage points in the proportion with good physical health and psychological and social wellbeing at end of the training in favour of the experimental group is close to the target difference of twenty, and the upper confidence limit for this difference reaches 30 percentage points. If there were to be a reduction in risk of two percentage points per session training attended, then it can be concluded that there is the potential for substantial benefits to prison inmates from sport participation.
Discussion
The study revealed that participation in sport (football) will develop quality of life (physical, social and psychological wellbeing) perceptions of inmates of Nigerian prisons. These results agree with previous findings that participation in sports inside prison are beneficial to inmate well-being in a number of ways such as reduced stress and frustration, alleviated boredom, increased self-esteem and a healthy routine, and development of social interaction and consequently friendships.9-11 Also, sport has been identified as a viable method of promoting physical, social and psychological wellbeing of general and clinical population and for reducing psychological and physical health risks among the general population.3-5 Some previous findings also showed that participation in outdoor sport among helped enhance inmate adjustment to their social environment and along with their social interactions.9 This adjustment is essential for achieving rehabilitative objectives during confinement through improvements in four broad areas: enhanced mood, stress reduction, a more positive self-concept, and a higher quality of life, which in turn reduces likelihood of recidivism or re-entry.28-33
It is therefore maintained that sport activities can be a vehicle for developing wellbeing, inclusion, acceptance and social skills.34-36 Sport involvement can be considered as an asset in rehabilitative programmes. Primarily, sport participation has positive effects on the general well-being of the prison population. Secondarily, providing inmates meaningful sports activities can help to reduce anti-social behaviours, offer a sense of belonging, provide opportunities to learn, reduce distances and increasing cohesion. Thus, by considering a prison like a social organization, sport-based programmes can effectively contribute to the development of the prison community’s social capital with a consequent advantage both for the prison community and for inmates as individuals. In conclusion, results of the study identified that improved quality of life is significantly associated to football skill acquisition and participation in the game by inmates of Ilesa and Ile-Ife prisons in Osun State, Nigeria.
Recommendations
Since research shows that prison inmates possess emotional, psychological and physical health challenges due largely to their confinement, their involvement in sport activities is therefore considered crucial for their social rehabilitation. Sport helps develop inmate quality of life, which includes physical fitness, self-esteem and healthy personality especially in resource-poor settings like those found in Nigerian prisons.
Sports in prison should provide inmates with years of opportunity for a regular and dedicated regimen of participation alongside recreational tournaments, which can adequately prepare them for post-release empowerment through sports.
There should be the regular organization of sport participation involving prison and the outside community in order to encourage more participation of inmates in community social contacts both inside and outside the prison, which is necessary to facility post-release community re-entry and social integration.
References
1. Mutrie, N and Biddle, S (1995) The Effects of Exercise on Mental Health in Non-Clinical Populations, Biddle, S. (ed) European Perspectives in Exercise and Sport Psychology, Champaign, Illinois, Human Kinetics
2. McAuley, E. and Morris, K.S (2006) Advances in Physical Activity and Mental Health: Quality of Life. American Journal of Lifestyle Medicine. Vol. 1 No. 5. 2007.
3. World Health Organisation (2003). Health and Development Though Physical Activity and Sport. Geneva, Wito Document Production Services.
4. Emily, B. K. (2002) The effectiveness of interventions to increase physical activity: a systematic review. American journal of preventive medicine, 22, 73-107;
5. American College of Sports Medicine (1995) Osteoporosis and Exercise: a position stand. MSSE, 27, 1-7;
6. Pérez-Moreno, F., Cámara-Sánchez, M., Tremblay, J. F., Riera-Rubio, V. J., Gil-Paisán1, L., and Lucia, A. (2007) Benefits of Exercise in Spanish Prison Inmates. Int J Sports Med 2007; 28: 1–7
7. Alemika. E. E. (1983) The Smoke Screen, Rhetorics and Reality of Penal Incarceration in Nigeria. International Journal of Comparative and Applied Criminal Justice, 7(1), 137-149.
8. Adesanya, A. (1995) A study of substance use and abuse among prison inmates. Dissertation for the award of the FMC psych of the West African postgraduate medical college.
9. Enuku-Evawoma U (1998) An analysis of the factors affecting the implementation of correctional education programmes in prisons in Edo/Delta States” Unpublished Doctorate Thesis University of Benin, Benin City, Nigeria.
10. Taminu, B (2010) ‘Nigeria Convicts and Prison Rehabilitation Ideals’ Journal of Sustainable Development in Africa (Volume 12, No.3, 2010). Clarion University of Pennsylvania, Clarion, Pennsylvania
11. Yelsma P and Yelsma J. (1977) Self-Esteem of Prisoners Committing Directly Versus Indirectly Destructive Crimes. Percept Motor Skills. 1977 Apr; 44(2):375-80
12. Rejeski WJ, and Mihalko SL. (2001) Physical activity and quality of life in older adults. J Gerontol A Biol Sci Med Sci. 2001; 56(special No. 2):23-35.
13. Chun, S., Lee, Y., Lundberg, N., McCormick, B., and Heo, J. (2008) Contribution of community integration to quality of life for participants of community-based adaptive sport programs. Therapeutic Recreation Journal, 42(4), 217-226.
14. Scientists (2010): Soccer improves health, fitness and social abilities.” PHYSorg.com. 6 Apr 2010. http://www.physorg.com/news189772740.html
15. Schomer, H.H. and Drake, S.B. (2001) Physical Activity and Mental Health. Int SportMed J. 2001;2(3). © 2001 International Federation of Sports Medicine
16. McAuley, E. and Morris, K.S (2006) Advances in Physical Activity and Mental Health: Quality of Life. American Journal of Lifestyle Medicine. Vol. X No. X. 2007.
17. Gould, D. (1986) Goal Setting for Peak Performance. In J. Williams (Ed.), Applied Sport Psychology (pp133-148). CA: Mayfield.
18. Shephard, R.J. (1998) Aging and Exercise. In: Encyclopedia of Sports Medicine and Science, T.D.Fahey (Editor). Internet Society for Sport Science: http://sportsci.org. 7 March 1998.
19. Williams, J. (1993) Applied Sport Psychology: Personal Growth to Peak Performance. (2nd ed.) CA: Mayfield.
20. Oladimeji, B. Y. (2005). Psychological Assessment Techniques in Health Care. Obafemi Awolowo University Press Limited, Ile-Ife, Nigeria.
21. Shumaker, S.A., Anderson, R.T. and Czajkowski, S.M. (1990) Psychological tests and Scales. In: Spilker, B. (Ed.) Quality of Life Assessment in Clinic Trials. Pp. 95-113. Raven Press, NY.
22. Naughton, M.J. and Shumaker, S.A. (1995) Assessment of Health-Related Quality of Life. In: Friedman, L., Furberg, C., 36. Demets, P. (Ed.) Fundamental of Clinic Trials. Pp. 185- 201. St. Louis, Mosby.
23. World Health Organization (1996) World Health Organization Quality of Life Assessment Instrument. Short Version (WHOQOL-Bref)
24. Medical Outcome Trust (1997) Clinical Practice Evaluation: World Health Organization and Quality of Life Measurement Instrument.
25. WHOQOL Group (1998) Development of the World Health Organization WHOQOL-BREF quality of life Assessment. Psychol Med 1998; 28: 551-8.
26. Sokoya (1999). Dissertation for the West Africa College of Physician, University College Hospital, Ibadan.
27. Ayeni, E.A (2002) The Post Treatment Psychosocial Functioning of Patients with Affective Disorders. M. Clinic Psychol. Thesis, Department of Mental Health, Obafemi Awolowo University, Ile-Ife.
28. Scottish Natural Heritage (2002) ‘The health, social, economic and environmental benefits of open-air recreation’, Scottish National Heritage. http://www.snh.org.uk/pdfs/access/rs-spbn.pdf (Information correct to April 2002).
29. Ryan, A. (1992) ‘Positive Gardening – The Benefits for Elderly People’, Growth Point, Summer 190.
30. Mattson, R. H. (1992) ‘Prescribing health benefits through horticultural activities’, in Relf, D. (ed) The Role of Horticulture in Human Well-Being and Social Development: A National Symposium. Timber Press, Portland, Oregon pp. 161 – 168.
31. United Nations office on Drugs and Crime (2009) ‘Handbook on Prisoners with Special Needs’, Criminal Justice Handbook Series, United Nations Publication No. E.09.IV.4; NY
32. Berger, B. (1996) ‘Psychological benefits of an active lifestyle: what we know and what we need to know’, Quest 48: 330 -353.
33. Hickman, S. A., Lee, R. E., Sallis, J. F., Castro, C. M. and Chen, A. H. (1999). The association of physical activity change with self-esteem in ethnic minority women: a prospective analysis’, Journal of Gender, Culture and Health 4 94): 281 – 292.
34. Bailey, R.P. (2004) Evaluating the Relationship between Physical Education, Sport and Social Inclusion, Educational Review, 56(3), pp. 71-90.
35. Coalter, F. (2005) The social benefits of sport: an overview to inform the community planning process. Edinburgh, Sport Scotland; Mead, G.H. (1934). Mind, self and society: from the standpoint of a social behaviourist. Chicago, University of Chicago press.
